60 year old female presents to the emergency department with increased pain in her right ear and decreased hearing. She denies ear discharge. She endorses vertigo for 7 months that is precipitated by sudden changes in head position. On physical exam, the right ear canal is obscured by a foreign body. Ear swab is positive for growth on fungal culture.
Lab Identification
Image 1. Salt and pepper fungal colonies isolated from ear swab.
Image 1. Salt and pepper fungal colonies isolated from ear swab.Image 2. Septate hyphae with unbranched condidiophore connected to a swollen vesicle covered in phialides that produce chains of conidia.
The identification of Aspergillus niger is made based on macroscopic colony morphology and microscopic structures. On the potato flake agar, Aspergillus niger grows salt and pepper colonies. For microscopic examination, a slide is made by touching the colonies with a piece of clear tape, putting a drop of lactophenol analine blue on a glass slide, and placing the tape on the slide. Microscopically, Aspergillus niger appears as septate hyphae with long smooth unbranched conidiophores. Compared with other Aspergillus species, the phialides of niger cover the entire vesicle and form a “radiate” head, which splits into several loose columns.
Discussion
Aspergillus is a common mold that lives both indoors and outdoors. The Aspergillus genus is composed of 180 species, among which 34 are associated with human disease.1A. fumigatus is the most common cause of aspergillosis syndromes. A. terreus is a species of particular concern due to its resistance to amphotericin. An invasive disease due to A. terreus has a poor prognosis.1
Healthy individuals inhale hundreds of conidia of Aspergillus per day without illness. However, people with a weakened immune system or lung disease are at higher risk of developing infections from inhaling the condidia. Presentations of aspergillosis range from allergy to fungal balls, to dissemination.1 Examples of aspergillosis include asthma, allergic bronchopulmonary aspergillosis, and allergic sinusitis.1
Invasive otitis externa due to Aspergillus is a rare, potentially life-threatening invasive fungal infection affecting immunocompromised patients.2 It spreads from the external auditory canal to adjacent anatomical structures such as soft tissues, cartilage, and bone.2 The condition can lead to osteomyelitis of the base of the skull with progressive cranial nerve palsies, irreversible hearing, and neurological impairment.2 The infection can be treated with antifungals.
References
Barnes PD, Marr KA. Aspergillosis: spectrum of disease, diagnosis, and treatment. Infect Dis Clin North Am. 2006 Sep;20(3):545-61, vi.
Parize, P. et al. Antifungal Therapy of Aspergillus Invasive Otitis Externa: Efficacy of Voriconazole and Review. Antimicrobial agents and chemotherapy. 2018 April; 62(4). http://aac.asm.org/content/53/3/1048.long
-Ting Chen, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 10 year old female presented to the pediatric emergency department (ED) with a chief complaint of persistent fever and chills for the past 10 days. Her mother reported the fevers reached up to 103°F and temporarily would respond to ibuprofen. She also noted a decrease in the patient’s appetite, tiredness and a bumpy rash on her truck and extremities. In the ED, she was clinically stable but her temperature reached a max of 104.7°F. On physical examination, shotty cervical lymphadenopathy was noted and there was no appreciable enlargement of the liver or spleen. Initial laboratory testing showed a white blood cell count of 10.6 TH/cm2 (normal range: 4.3-11.4 TH/cm2) and elevated acute phase proteins (ESR 45 mm/HR and CRP 2.6 mg/dL). Blood cultures were collected and the patient was started on ceftriaxone. Pediatric infectious disease was consulted and a thorough infectious work up was completed.
Laboratory Identification
Rapid influenza antigen test: Negative
Rapid Group A Strep antigen test: Negative
Rapid Monospot: Negative
HIV antigen/antibody (4th generation) test: Negative
Legionella urinary antigen: Negative
Histoplasma urinary antigen: Negative
Antinuclear antibody: Negative
Rheumatoid factor: Negative
Urine culture: Negative
Blood cultures: Negative
Bartonella henselae IgM: ≥1:20 (normal <1:20)
Bartonella henselae IgG: ≥1:1024 (normal <1:128)
Infectious disease and rheumatologic work ups, as listed above, were negative with the exception of a positive IgM and IgG serologic testing for Bartonella henselae, with the results suggesting a recent infection based on the elevated titers. Upon further questioning, the family did have many outdoor cats and dogs; however, the child denied any recent bites or scratches.
Discussion
Bartonella henselae is a facultative, Gram negative coccobacillary rod that is the causative agent of cat scratch disease and bacillary angiomatosis. The main reservoir for B. henselae is cats and the disease is spread from cat to cat via the cat flea. Feral cats, outdoor cats and young kittens, especially those living in hot, humid environments where fleas are plentiful, are more likely to be infected and spread the disease to humans via infective flea feces during a scratch or bite from the cat.
The incubation period for B. henselae ranges from 1-3 weeks and the majority of patients present with systemic symptoms including fever, chills, malaise, anorexia and headache. In addition, painful lymphadenopathy, on the side of the body where the scratch occurred (most common upper extremity), can be present in the epitrochlear, axillary and cervical regions. Less frequently, B. henselae causing bacillary angiomatosis can result in the proliferation of vessels in organs (liver and spleen). Though rare, encephalopathy and endocarditis due to B. henselae are the most severe manifestations of disease.
In the microbiology laboratory, the diagnosis of B. henselae is challenging due to the fact it is slow growing, highly hemin dependent and requires high humidity conditions for growth. The organism will grow on chocolate and heart infusion agars containing 5% fresh rabbit blood. Plates should be incubated at 35°C with 5% CO2 with high humidity for at least 4 weeks. Colonies are irregular and off-white in color and B. henselae is negative for both catalase & oxidase and asaccharolytic.
Due to the identification difficulties with culture, serologic testing is the main methodology for the diagnosis of B. henselae. Enzyme linked immunosorbent assays (ELISA) are relatively easy to perform and provides good results, although the provider should be aware of the sensitivity of the particular platform, the fact that cross reactivity with other Bartonella spp. can occur and seronegative infections can sometimes occur. Warthin-Starry silver stain on fixed tissue sections from lymph nodes and other organs can be helpful as well; however, it is relatively insensitive and not highly specific.
With regards to treatment, there are no agreed upon breakpoints for B. henselae published by CLSI or EUCAST. Microdilution or Etests can be used for testing and isolates have been susceptible to many antibiotics. In general, for cat scratch disease, it does not respond to antibiotic therapy and there is only a minimal benefit of antimicrobial agents. In the case of our patient, she was switched from ceftriaxone to a five day course of azithromycin with a gradual improvement of her fever curve. She was scheduled to follow up with pediatric infectious disease in 2-3 weeks.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
In parts 1 and 2, we discussed pre-analytical and analytical issues that can be faced when culturing tissue specimens. Part 3, the final part of the Tissue is the issue series, will review analytical and post-analytical issues of tissue culture requests.
The Issue
Let’s consider a case of “culture-negative” endocarditis (1), in which organism was detected during direct observation of the specimen (2); but as you would expect for suspected “culture-negative” endocarditis, the culture does not yield an organism. This can happen for a variety of reasons. Perhaps the culture request was for a routine aerobic culture, but the organism was a strict anaerobe and therefore could not grow. Maybe the patient was on antibiotics, so the organism observed was not viable. Or it is possible that the organism in question is fastidious and requires special media or growth conditions which were not met. Another frequent occurrence is that tissue is sent for pathology, but not for culture. This is more common when malignancy is expected, but the pathological findings suggest an infectious process. These scenarios may seem hopeless, but don’t despair; there is a non-culture alternative that can aid in identifying the causative agent.
The Solution
Microbial (bacterial, fungal, and viral) DNA can be detected from fresh, frozen, or fixed tissue. Simply put, DNA is first extracted from the specimen, of which the microbial DNA of interest (bacterial, fungal, viral) is then amplified via PCR. Broad-range or pathogen-specific PCRs are commonly available from a variety of reference laboratories. If broad-range PCR is performed, then sequencing of the amplicon is required to determine the organism identification. Sequences are queried against a library of known microbial genomes to obtain a match.
Depending on the DNA of interest, different primer sets are utilized. For broad-range bacterial PCR, the 16S ribosomal RNA gene is typically used. Although mycobacteria are bacteria, they require additional gene targets for optimal detection and identification (16S rRNA, rpoB, and hsp65). For fungi, the 28S rRNA and the ITS (internal transcribed spacer; ITS1 and ITS2) genes are used.
The organism burden and specimen type can affect the probability of detecting an organism and obtaining its identification. The likelihood of a positive outcome is proportional to the organism burden. For example, if organism observed in the direct exam (i.e., Gram or acridine stain), then the organism can usually be detected and identified. However, if no organism is observed, then the chances of a positive result is unlikely. Therefore, our protocol is to only send specimens for microbial DNA sequencing on specimens in which organisms were observed in the direct exam. This is true for all specimen types (fresh, frozen, fixed).
It is important to note that fixed specimens may not yield as good results as a fresh or frozen specimen. This is because the process of fixation can degrade the microbial DNA (3). Additionally, because detection of microbial DNA is the basis for pathogen identification, susceptibility results are not going to be available. Treatment options will need to be based on known empiric therapies.
The Conclusion
Microbial DNA sequencing is a viable option for the identification of etiological agents of infection from a variety of sources, such as culture-negative infections. Other uses include slow-growing organisms and organisms that are unidentifiable by traditional methods (4). In my experience, this is a valuable tool that should be considered when culture does not yield a result and a result is necessary to drive clinical decisions.
Martinez, R.M. Genes in your tissue: probe identification and sequencing microbial targets from formalin-fixed, paraffin-embedded tissue. Clin. Microbiol. Newslett. 36: 139-147.
-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
An 88 year old male presents with fever, nausea, and headache. The patient reported a diffuse headache accompanied by malaise, fatigue, and nausea without vomiting. He denied confusion, irritability, or a personal and family history of headaches. According to the patient, he frequently attends cookout parties and enjoys fruits, salads, wine, and cheese. Temperature is 38.2 degrees Celsius, blood pressure is 96/65 mmHg, pulse is 102 beats/minute, and respiratory rate is 20 breaths per minute. Physical exam is negative for nuchal rigidity and Kernig sign. Funduscopic exam is negative for papilledema. CBC shows leukocyte count of 16,000/mm3. The patient’s blood culture is positive.
Laboratory Identification
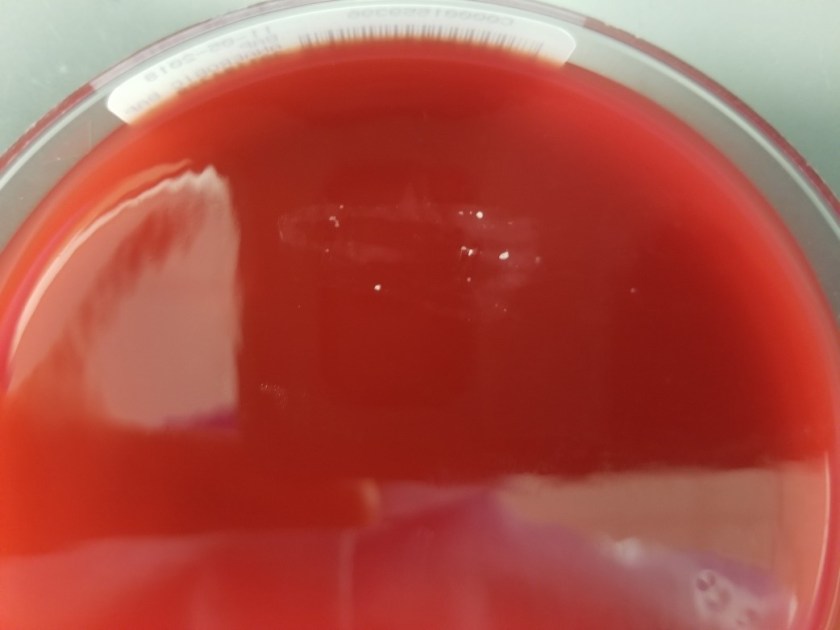
Image 1. Short gram positive bacilli identified on Gram stain of blood culture (100x oil immersion).Image 2. Aerobic growth of round and translucent colonies with a narrow zone of beta hemolysis subcultured from positive blood culture bottle to sheep blood agar plate.
The blood culture was positive for short, gram positive bacilli. Sheep blood agar plate grew round and translucent colonies which have a narrow zone of beta hemolysis as shown on our plate. The organism was catalase positive and motile at 25 degrees Celsius. It showed end over end tumbling motility in a wet prep and an umbrella pattern in semi-solid motility medium. It was identified by MALDI-ToF as Listeria monocytogenes.
Discussion
Listeria monocytogenes is a gram positive bacillus that is isolated from the environment and a variety of animals. It is associated with foodborne outbreaks from dairy and meat products. The most common foods associated with listeriosis outbreaks include unpasteurized raw milk, cold deli meat, hot dogs, raw sprouts, smoked seafood, and soft cheese.1
Listeria commonly infects pregnant women, immunocompromised individuals, and elderly 65 years or older.1 Among pregnant women, Listeria can lead to miscarriages, stillbirths, and newborn meningitis resulting in death.1 In 1985, an outbreak of Listeria due to soft cheese resulted in 142 individuals sick, 10 newborn deaths, 18 adult deaths, and 20 miscarriages.1 Among the immunocompromised and elderly, Listeria can cause septicemia and meningitis. In 2011, a cantaloupe outbreak due to Listeria resulted in 147 people sick in 28 states and 33 deaths.1 The infected population was mostly over the age of 65 years.1 In addition, Listeria can cause acute febrile gastroenteritis in healthy individuals.2 Patients typically present with fever, watery diarrhea, nausea, headache, and pain in joints and muscles.2 Symptoms start 24 hours after the ingestion of bacteria and resolve by themselves in 2 days.2
Treatment of Listeria depends on the severity of symptoms. Although pregnant women with Listeria infection typically present with a self-limited flu-like illness, they are treated with IV ampicillin to prevent infection of the fetus.1 For patients other than pregnant women, the treatment of Listeria infection depends on the severity of symptoms.
Say Tat Ooi, Bennett Lorber; Gastroenteritis Due to Listeria monocytogenes, Clinical Infectious Diseases, Volume 40, Issue 9, 1 May 2005, Pages 1327 1332, https://doi.org/10.1086/429324
-Ting Chen, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
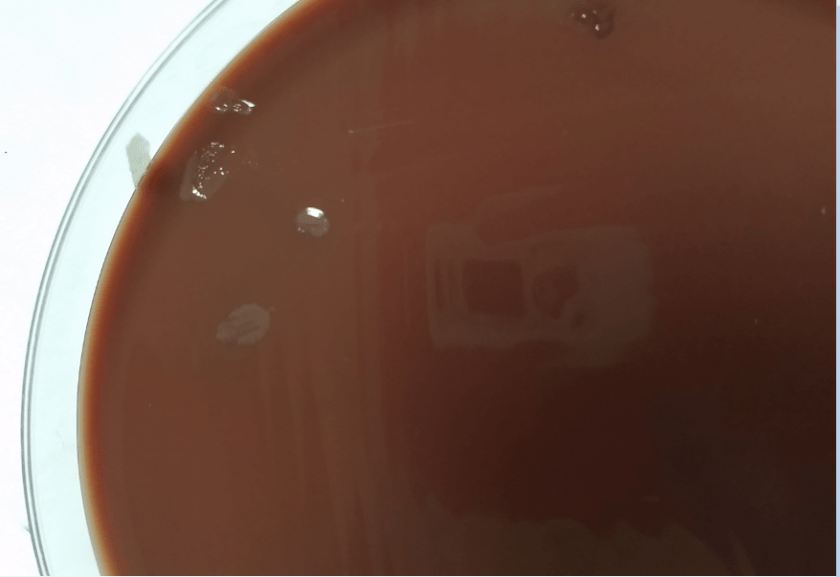
Our patient is a 45-year-old female who presents to the Emergency department with breast pain. She was diagnosed with granulomatous mastitis 3 months prior. She was treated with 3 weeks of steroids, but they were stopped when the mass was unchanged and the patient was experiencing increasing breast tenderness. Since then she and has undergone several procedures to drain her right breast abscess, the most recent being five days prior. The woman has been treated with sequential courses of sulfamethoxazole–trimethoprim and metronidazole without improvement. On this visit, the abscess was again drained and sent to the microbiology laboratory for culture. The Gram stain showed no bacteria and 3+ polymorphonuclear cells. After 48 hours incubation there was scant growth on the blood agar plate and no growth on the chocolate, MacConkey or CNA plates. The colonies growing on the blood plate were tiny, white, and lipophilic (Image 1).
Image 1. Small, white, lipophilic colonies growing on blood agar plate at 48 h incubation. There was no growth of this organism on chocolate or MacConkey agars this time point.
Discussion
The organism was identified as Corynebacterium kroppenstedtii.
Colonies on the blood agar plate were identified as Corynebacterium kroppenstedtii using MALDI-TOF mass spectrometry for identification. C. kroppenstedtii is catalase positive, non-motile and a facultative anaerobe. It grows better on 5% sheep blood agar than chocolate agar, as is the case for many Corynebacterium spp. Corynebacterium come in two varieties, lipophilic such as Corynebacterium jeikeium, and luxuriantly growing, such as Corynebacterium straitum. C. kroppenstedtii is part of the former lipophilic group, forming small colonies after extended incubation. Lipids such as Tween-80 can added to the media to improve growth of lipophilic Corynebacterium such as C. kroppenstedtii, but clinically this is not routinely performed. When viewed on a gram stain, the bacteria are rod-shaped gram positive diptheroids with typical coryneform morphology. Both MALDI-TOF and 16S rRNA sequencing can accurately identify C. kroppenstedtii to the species level.
C. kroppenstedtii is a relatively newly recognized species within the Corynebacterium genus. It was first described in a case series of young Polynesian women with histological evidence of lobar mastitis, from which C. kroppenstedtii was identified from >40% of the patients’ abscesses. Since that time, isolation of C. kroppenstedtii has been clinically associated with breast abscesses and granulomatis mastitis. C. kroppenstedtii is a highly lipophilic bacterium. Its cell wall lacks many mycolic acids, which may explain its propensity to grow in lipid-rich sites such as mammary glands. C. kroppenstedtii typically affects women of reproductive age and can be difficult to diagnose due to the slow growing nature of the lipophilic organism and the relatively few organisms present in abscess specimens.
Prior to identification by MALDI-TOF MS and 16s rRNA sequencing this patient’s culture would have been reported as rare or 1+ “dipthroid,” “coryneform,” or “Corynebacterium spp.” Without knowing the clinical significance of this organism, the culture results could easily be dismissed as contaminating skin flora.
It is very difficult to treat C. kroppenstedtii in abscesses, with the most effective treatment requiring both surgical drainage of the abscess and long term antibiotic use. It is fairly difficult to get antibiotics to the site of infection, so antibiotics that test as susceptible in the laboratory may not eradicate the pathogen. Our patient’s isolate of C. kroppenstedtii was susceptible to ciprofloxacin, clindamycin, doxycycline, and intermediate to penicillin. She remains on ciprofloxacin therapy, but has ongoing right breast tenderness. She had another surgical drainage of her breast abscess a week after this case, and the culture also grew 1+ C. kroppenstedtii with 3+ PMN seen on Gram stain, so her infection has not yet been resolved. References
Tauch, Andreas, et al. “A Microbiological and Clinical Review on Corynebacterium Kroppenstedtii.” International Journal of Infectious Diseases, vol. 48, 2016, pp. 33–39., doi:10.1016/j.ijid.2016.04.023. ScienceDirect.
Johnson, Matthew G., et al. “The brief case: recurrent granulomatous mastitis due to Corynebacterium kroppenstedtii.” Journal of clinical microbiology 54.8 (2016): 1938-1941.
Paviour, Sue, et al. “Corynebacterium species isolated from patients with mastitis.” Clinical Infectious Diseases 35.11 (2002): 1434-1440.
-Carolyn Wiest, MT(ASCP) graduated from Michigan State University with a BS in molecular genetics and is a medical technologist at NorthShore University HealthSystem. Her interests are in microbiology and molecular diagnostics.
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois.
A 28 year old female with a history of Ulcerative Colitis on humira and azathioprine presented with proctitis and a recent perirectal abscess. The patient reported a two week history of progressively worsening pain and swelling in the perianal region. In addition, she reported recent purulence excreted with bowel movements. On physical exam, the patient was afebrile and negative for rash, oral lesions, joint pain, or abdominal pain. A perirectal abscess was identified and drained. Abscess culture was positive. Patient reported recently engaging in high-risk sexual behavior with multiple male sexual partners often without protection.
Lab Identification
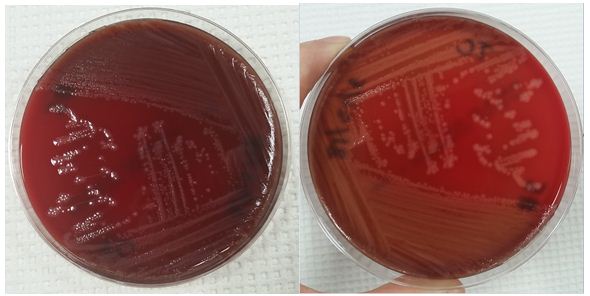
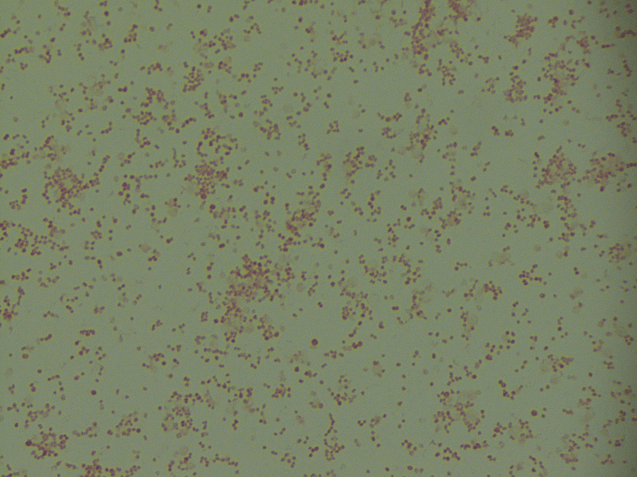
Image 1. Kidney-bean shaped gram negative cocci identified on Gram staining of perirectal abscess culture (100x oil immersion). Image 2. Aerobic growth of flat, gray-white, and moist colonies from perirectal abscess on chocolate agar plate.
Abscess culture grew kidney-bean shaped gram negative diplococci. Colonies on chocolate agar plate appeared medium sized, flat, gray-brown, and moist. The organism was oxidase positive and identified by MALDI to be Neisseria gonorrhoeae.
Discussion
Neisseria gonorrhoeae is a kidney-bean shaped gram negative diplococci for which humans are the only host. The organism causes gonorrhea, a common sexually transmitted disease, among young people between the ages of 15-24 years. Gonorrhea is spread by sexual contact or through the birth canal. The most common site of infection is the urogenital tract.2 Males commonly present with dysuria with penile discharge.2 Females commonly present asymptomatically or with symptoms such as mild vaginal mucopurulent discharge and severe pelvic pain2. In addition, gonorrhea can cause infections of the anus, conjunctiva, pharynx, ovary and uterus.2 In the neonate, the culprit organism can lead to ophthalmia neonatorum.2 Lastly, gonorrhea causes disseminated disease such as arthritis, endocarditis, meningitis, and skin lesions on extremities.2 CDC currently recommends treating gonorrhea with dual therapy, a single dose of 250 mg intramuscular ceftriaxone and 1g of oral azithromycin.1
Antibiotic resistance in gonorrhea is an increasing public health concern. The World Health Organization has a program that monitors the global antimicrobial resistance of gonorrhea.3 The data from 77 countries between 2009 and 2014 showed that 66% of reporting countries had encountered gonorrhea strains with either resistance or reduced susceptibility to ceftriaxone.3 81% of reporting countries had encountered gonorrhea strains resistant to azithromycin.3 Given these data, it is important to improve gonorrhea prevention and continue to monitor gonorrhea antibiotic resistance at both the national and global levels.
Miller KE. Diagnosis and Treatment of Neisseria gonorrhoeaeAm Fam Physician. 2006 May 15:73 (10): 1779-1784.
Wi T, et al. Antimicrobial resistance in Neisseria gonororheae: Global surveillance and a call for international collaborative action. PLoS Med 14(7): e1002344.https://doi.org/10.1371/journal.pmed.1002344
-Ting Chen, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
Most laboratories (and clinicians) utilize and rely on microscopic observation as the first step in the detection and identification of microorganisms. In some cases, direct microscopic analysis is used to determine the immediate clinical course of action. For example, if during a surgical procedure infection is suspected, then it is possible for the surgeon to submit a specimen to the laboratory for rapid (STAT) analysis. If polymorphonuclear leukocytes (PMN) and organisms are observed, then the differential diagnosis of infection is confirmed. Assuming proper specimen collection; if no PMN and no organisms are seen, then infection is less likely (true in most cases; there are always exceptions). These direct microscopic observation results thus drive the surgeon’s decision to either remove the infected area or perhaps advises on the use of intraoperative antimicrobials.
In part 1 of this series we discussed the pre-analytical problems associated with tissue culture; specifically, how specimen processing can affect whether or not organism is detected and recovered (1). In part 2 we will consider methods used for the direct observation of microorganisms in tissue specimens.
The Issue
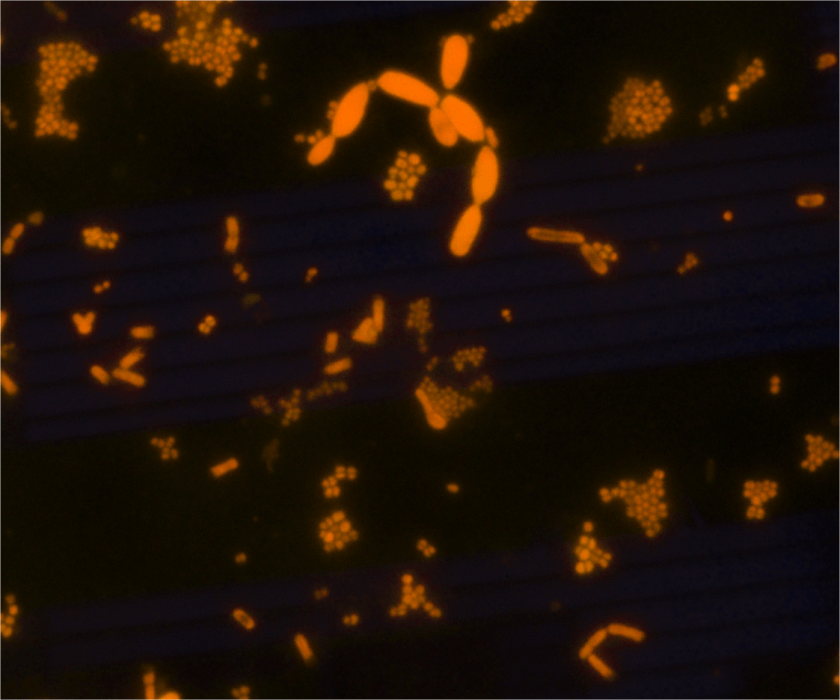
Let’s take a step back to review our previous “culture-negative” endocarditis case (1). Recall that the blood cultures were negative at first, no organisms were observed on the Gram stain and the culture was also negative of the valve tissue. However, when we evaluated the frozen tissue that was “split” and saved for sequencing, the organism was observed via acridine orange (AO).
Image 1. AO of a positive broth culture from a homogenized tissue specimen. The AO stain displays cocci, bacilli, and yeast. The DNA-containing cells fluoresce orange.
The Solution
AO is a fluorescent dye that intercalates nucleic acids. It is a rapid, inexpensive, and most importantly- it is a sensitive alternate dye that can aid in microorganism detection in a variety of specimen types (2, 3 ,4, 5). AO is more specific than Gram stain (2, 3). Because bacterial DNA is not contained in a nucleus, but freely contained within the cell, the AO-stained cell takes the shape of the organism’s cellular morphology (Image 1). For example, if the organism is Staphylococcus aureus, then the AO would exhibit Gram positive cocci in clusters. Similarly, if the organism in question is Escherichia coli, then Gram negative bacilli would be observed, etc.
Some organisms (Campylobacter, Mycoplasma, etc.) do not stain well with Gram stain and as such they can be difficult to detect in direct specimen observations. The presence of many PMN and no organisms may be a clue that the organism is present in low numbers or that the organism does not stain well with the Gram stain. In cases such as these, the use of AO has proven to be very useful. Additionally, if the morphology of an organism in a Gram stain is difficult to interpret, then AO can also provide a more clear-cut answer. Lastly, the presence of artifact(s) can be problematic when reading Gram stains. “Is that Gram positive cocci or junk?”. Junk usually does not contain DNA and therefore does not fluoresce. Therefore, the information provided by the AO stain can aid in your decision to report cocci or not.
One disadvantage is that a fluorescent microscope is required to visualize the stain. Implementing AO may require the purchase of new equipment as not all laboratories have access to a fluorescent microscope. Because AO stains nucleic acid, anything with DNA or RNA will stain positive. This is another disadvantage because too much material that is positively stained can make interpreting the stain difficult at times. Another disadvantage is that a Gram stain is still required because the AO only allows the visualization of DNA-containing cells, it does not determine the Gram stain reaction.
Thinking back to our original case, the organism was present in the frozen tissue piece. It was not detected in the direct Gram stain, but rare organisms were noted in the AO. Because the AO was positive, we then reviewed the Gram stain and found rare Gram negative bacilli. This suggests that the organism was initially missed in the Gram stain because of the low abundance present. Bottom line, the AO was positive and we were thus able to provide the clinical team with relevant information.
The Conclusion
There are many stains used to aid in the observation of microorganisms. The AO stain is easy to perform, inexpensive, rapid, sensitive, and versatile. AO can be used on direct specimen smears, isolated colonies, and formalin-fixed paraffin embedded sections. Although there are limitations to using AO, the benefits considerably outweigh the shortcomings. AO is a great tool that laboratories should consider implementing as an alternate method for the direct observation of microorganisms.
Mirrett, S., Lauer, B.A., Miller, G.A., and Reller, B. 1982. Comparison of Acridine Orange, Methylene Blue, and Gram stains for Blood Cultures. J. Clin Microbiol. 15; 4: 562-566.
Lauer, B.A., Reller, B., and Mirrett, S. 1981. Comparison of Acridine Orange and Gram Stains for Detection of Microorganisms in Cerebrospinal Fluid and Other Clinical Specimens. J. Clin Microbiol. 14; 2:201-205.
Martinez, R.M., Bowen, T.R., and Foltzer, M.A. Prosthetic Devise Infections. Diagnostic Microbiology of the Immunocompromised Host. 2016 (Book chapter, chapter 27. Pages 711- 733. ASM Press.
Cooper, J.D., Dometita, D., Hasan, A., Dorion, P., Wolk, D.M. and Martinez, R.M. Orange you glad you checked the buffy coat? Clin. Microbiol. Newslett. 37: 9-13.
-Raquel Martinez, PhD, D(ABMM), was named an ASCP 40 Under Forty TOP FIVE honoree for 2017. She is one of two System Directors of Clinical and Molecular Microbiology at Geisinger Health System in Danville, Pennsylvania. Her research interests focus on infectious disease diagnostics, specifically rapid molecular technologies for the detection of bloodstream and respiratory virus infections, and antimicrobial resistance, with the overall goal to improve patient outcomes.
A 27 year old African American male presented to the emergency department with confusion and abdominal pain. His past medical history was significant for a 100 pound unintended weight loss and oral candidiasis which prompted a recent diagnosis of HIV. He was prescribed anti-retroviral therapy and antibiotic prophylaxis with which he reported compliance. Currently, he had no fever or chills. An abdominal CT scan showed an enlarged liver & spleen, generalized lymphadenopathy and a small amount of fluid. Significant lab work included anemia with a platelet count of 18,000 TH/cm2, absolute CD4 100 cells/cm2 (reference range: 506-3142 cells/ cm2) and a HIV viral load of 4,871 vc/mL. Given the concern for an infectious process, the infectious disease service was consulted and the patient underwent a thorough infectious work up including lumbar puncture, was started on board spectrum antibiotics and antifungals and was placed in airborne isolation until Mycobacterium tuberculosis could be ruled out.
Laboratory Identification
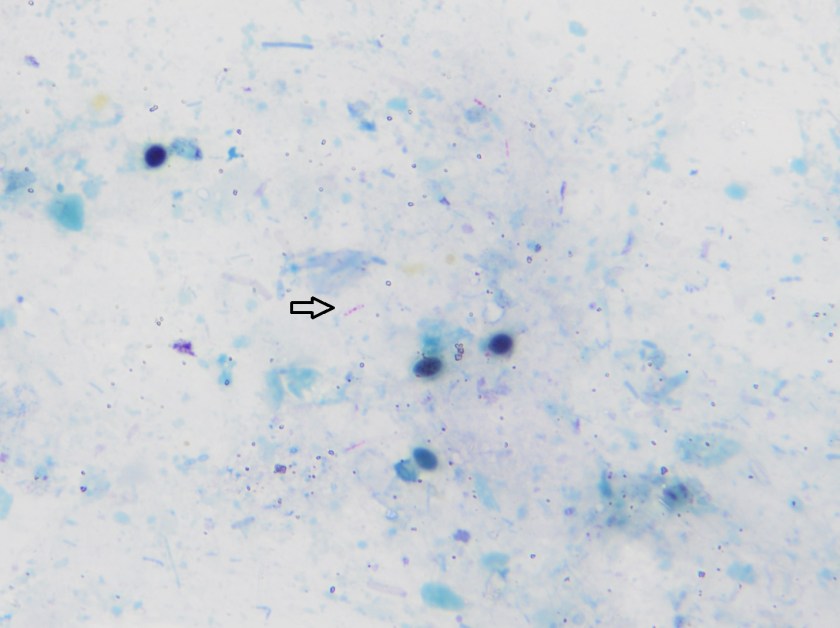
Image 1. Direct smear from a stool specimen showed beaded acid fast bacilli (Kinyoun stain, 1000x oil immersion).Image 2. Direct smear from a stool specimen showed beaded acid fast bacilli (Kinyoun stain, 1000x oil immersion).
Initial diagnostic testing for bacterial, fungal and viral pathogens was negative. Three concentrated sputum AFB smears as well as a TB PCR were negative. The quantiferon gold TB test was also negative. The physician additionally ordered AFB blood and stool cultures. The direct smear from the stool specimen showed rare, beaded acid fast bacilli in a background of bacteria and yeast normally present in the stool via Kinyoun stain (Images 1 & 2). The specimen was sent to the department of health for additional work up. There was growth after 21 days incubation and Mycobacterium avium complex was identified by high performance liquid chromatography (HPLC).
Discussion
Mycobacterium avium complex (MAC) is a slow growing nontuberculous mycobacteria (NTM) frequently involved in human disease. Historically, it was classified as Runyon group III which are non-chromogens and do not produce pigment regardless of culture conditions. The group encompasses two taxa, M. avium and M. intracellulare. The species M. avium can further be classified into four subspecies: subsp. avium, subsp. silvaticum, subsp. paratuberculosis and subsp. hominissuis. Of interest, M. avium subsp. paratuberculosis can often be seen in association with Crohn’s disease.
In general, MAC organisms have low pathogenicity, but in the setting of those with lung disease (including cystic fibrosis), heavy smokers, immunocompromised patients and those with HIV, it is a well-known cause of disease. Infections with MAC can range from localized mycobacterial lymphadenitis and isolated pulmonary disease to bacteremia with dissemination to almost any organ. The organisms are located in circulating monocytes and further spread most commonly to the lungs, gastrointestinal tract and lymph nodes. In the case of HIV positive patients, MAC is the most common environmental NTM causing disease, especially in those with CD4 counts less than 100 cells/mm3 who are more likely to have disseminated disease.
In order to diagnosis MAC infections, specimens from blood, sputum, lymph nodes and other tissues are preferred. In addition, stool may also be an acceptable alternative in HIV patients if other specimens are negative or unable to be obtained. However, the sensitivity of a direct stool smear is only 32 to 34% making it not a very effective approach to identifying those at risk for disseminated infections. Once the culture has growth, various methods can be used to identify MAC, including phenotypic methods, DNA probe testing, HPLC, pyrosequencing and other forms of PCR & sequencing.
In the case of our patient, he was started on M. tuberculosis therapy: rifabutin, isoniazid, pyrazinamide & ethambutol (RIPE) until TB was ruled out. At that time, he was removed from isolation and switched to a drug regimen that included azithromycin, rifabutin and ethambutol. He showed clinical improvement and his cell counts, renal function and liver enzymes trended to normal ranges.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.
Our patient is an 83 year old female with previous history of arterial hypertension, atrial flutter and chronic obstructive pulmonary disease who presented with dry cough (~2 weeks), fever (102ºF), and cutaneous ulcerated plaques with elevated borders on forearm, foot, leg, and neck. Chest radiographs and chest CT scan showed numerous bilateral nodular consolidations compatible with pneumonia. Additionally, mild leukocytosis (14,200 cells /mm3) and hypohemoglobinemia (10.9 mg/dl) were documented. A skin biopsy was taken from the forearm lesion. Periodic acid–Schiff (PAS) and Grocott-Gomori’s (or Gömöri) methenamine silver (GMS) stains identified rare budding yeast (PAS, Image 1). Acid-fast bacilli (AFB) and Gram stains were negative for mycobacteria and bacteria, respectively.
Image 1. Budding yeast with a thick double cell wall were identified microscopically surrounded by prominent supurative granulomatous reaction (PAS, 100x).
Discussion
A diagnosis of disseminated blastomycosis was made based broad based budding yeast seen on PAS stain (Image 1).
Blastomycosis infection most commonly affects persons living in the Mississippi and Ohio River valleys, Great Lakes Region of the United States, and southern Canadian provinces. It is a fungal infection that can cause asymptomatic infection, isolated pulmonary disease, or serious and potentially fatal disseminated disease. B. dermatitidis can infect every organ of the body giving great variety of clinical manifestations, which is the reason why it is known as “the great pretender.” More than half of infected patients are asymptomatic. Symptomatic patients generally present with pulmonary symptoms, and the development of disseminated disease after hematogenous spread is common (~25 to 40% of symptomatic cases). The most common extra-pulmonary locations are: skin, bone, genitourinary tract, and central nervous system (CNS). Unlike histoplasmosis, most cases of blastomycosis are seen in immunocompetent patients, although immunocompromised patients may be at higher risk to develop severe forms of the disease.
Blastomyces is a thermally dimorphic fungus that grows as a yeast in the body and as filamentous fungi with septate hyphae in the environment. Recent phylogenic analysis has divided the Blastomyces genus into 2 species, B dermatitidis and B gilchristi . Culture of B. dermatitidis from the environment is extremely difficult, and much of what we know is conjecture from a few documented outbreaks, of which several occurred in wooded areas near waterways. These investigations found that exposure to dust clouds associated with construction or crop harvesting were the only identified risk factors for infection. Blastomycosis infection occurs through aerosolization of conidia from the environment causing respiratory infection or less commonly through direct inoculation into cutaneous abrasions. Once in the host, the conidia transform into yeast. The specific proteins expressed during the yeast phase allow the evasion of phagocytic and CD4+ cells.
Laboratory diagnosis
The most expedient method to diagnose blastomycosis remains examination of stained fluid or tissue specimens. Yeast are 8-15 µm in size with broad based buds of 4-5 µm and have a characteristic refractory double cell wall. Fluid can be stained with 10% potassium hydroxide plus calcofluor white, whereas formalin fixed paraffin embedded tissue samples can be stained with GMS or PAS. B. dermatitidis yeast can be difficult to visualize with Gram or hematoxylin and eosin (H&E) stains, but if found, the characteristic broad-based budding pattern of yeast can lead to presumptive diagnosis before culture and non-culture based diagnostic test results are available.
Culture of B. dermatitidis provides a definitive diagnosis of pulmonary and extra-pulmonary disease. B. dermatitidis grows well on routine fungal media such as Sabouraud dextrose agar, potato dextrose agar, and brain–heart infusion media. The yeast phase is inhibited by media containing cyclohexamide. Culture typically demonstrates growth in as little as 4-7 days. Colonies will initially appear yeast-like, but then develop white cottony aerial mycelium and turn tan with age. Mature growth is achieved around day 14 and the reverse of the colony is a tan color. At 25-30°C, B. dermatitidis forms septate hyphae with round or pear-shaped conidia attached to the hyphae by short or long conidiophores. This gives the characteristic appearance of “lollipops.” Scedosporium spp. and Chrysosporium spp. are common confounders because they make similar structures. Definitive identification of Blastomyces sp. can be made by conversion of the mold phase to the yeast phase by incubation at 37°C. An alternative to conversion is using a DNA probe assay.
References
Medically Important Fungi, 5th edition
Principles and Practices of Infectious Disease, 7th edition
-Julio Diaz-Perez, MD is a 1st year anatomic and clinical pathology resident at University of Chicago (NorthShore).
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois.
A 42 y/o female G2P2002 patient presented to her Ob/Gyn for Colposcopy for monitoring of persistent High-Risk HPV. She was originally found positive for HPV in 2015, but has had never had a Pap with a squamous intraepithelial lesion, abnormalities on colposcopy, or dysplasia seen on endocervical curettage. Additionally, she endorsed a complaint of vague diffuse pelvic/lower abdominal pain for approximately the last 2 months. She states that the pain is mild and comes and goes and is not associated with anything in particular. She has noticed some clear to gray-white discharge now and then since she first noticed the pain, but nothing that really worried her. Pt denies changes in bowel or bladder habits, denies nausea, fever, or chills. Pt has been in a monogamous relationship with her partner for the last 12 years. She had a Mirana IUD placed 4 years prior, without complication, and has not had menses since placement. Prior to that, the patient had normal, regular cycles. She has 2 children with the same father, both were delivered by spontaneous vaginal delivery without complications. She has mild anxiety and depression for which she is treated, but no other medical problems. There is no surgical history. She has 1-2 glasses of red wine every week, denies tobacco use, and denies illicit drug use.
Pelvic exam revealed a benign appearing cervix that was not painful to touch or motion. There was a clear to white mild discharge that was suspected to be normal vaginal secretions. IUD strings were noted. Colposcopy revealed an easily appreciated transformational zone without any obvious lesions. A routine endocervical curettage (ECC) was performed followed by observed increased clear discharge from the cervical os. ECC was sent for routine pathology:
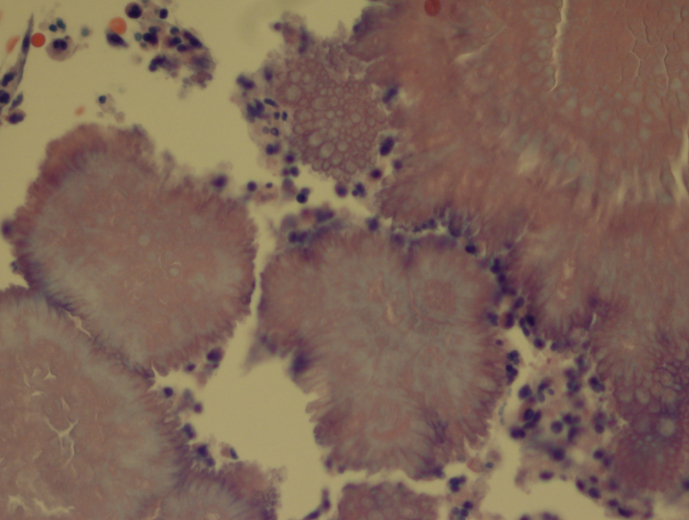
Actinomyces, H&E, 20xActinomyces, H&E, 40x
Discussion
Actinomycosis is an infection by a species within the Actinomyces genus, generally seen in dental and other oropharyngeal abscess formations. However, rare occurrences of pelvic Actinomycosis can be seen in women with intrauterine devices in place. Pelvic infections can result in cervicitis and endometritis and progress into abscess formation within the fallopian tubes and the ovaries along with salphigitis. The more profound disease consisting of abscess formation generally presents with fever, specific lower abdominal tenderness, and elevated WBCs, thus can mimic acute appendicitis, ovarian torsion, or ectopic pregnancy (1). The first case reported in the literature was in 1967 (2).
Three main species of Actinomyces have been found to be associated with IUD-associated pelvic infection: A. naeslundii, A. odontolyticus (3), and A. hongkongensis (4). All of these species are obligate to facultative anaerobes, catalase negative, and nitrate reducing. A sub-species group of A. naeslundii, however, can be catalase positive and is CAMP test-positive. All members of A. naeslundii are urease positive while A. odontolyticus and A. hongkongensis are urease negative.
References
Joshi et al. Pelvic Actinomycosis: a Rare Entity Presenting as Tubo-ovarian Abscess. Arch Gynecol Obstet. 2010, 281:305-306.
Brenner et al. Pelvic Actinomycosis in the Presence of an Endocervical Contraceptive Device. Obstet Gynecol. 1967, 29: 71-73.
Woo et al. Diagnosis of Pelvic Actinomycosis by 16S ribosomal RNA Gene Sequencing and its Clinical Significance. Diagnostic Microbiology and Infectious Disease. 2002; 43: 113-118.
Flynn et al. Identification by 16S rRNA Gene Sequencing of an Actinomyces hogkongensis Isolate Recovered from a Patient with Pelvic Actinomycosis. J. Clin. Microbiol. 2013, 51(8):2721. DOI: 10.1128/JCM.00509-13.
-Jeff Covington, MD, PhD, is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.