A 64 year old female with metastatic left breast cancer,
status-post chemotherapy, presented for erythema, discomfort, and oozing from
her port site for approximately one month. At presentation she was afebrile.
Her port site exhibited erythema and fluctuance. Her most recent absolute
neutrophil count was 1910/cmm. Her port was removed, and a tissue specimen was
sent for microbiologic examination.
Laboratory
Identification
Gram stain showed neutrophils without bacteria. Aerobic
cultures grew a beaded gram positive rod on blood agar at 36 hours. Kinyoun
stain was positive for acid fast bacilli. Matrix assisted laser desorption
ionization-time of flight mass spectrometry (MALDI-TOF) at that time identified
Mycobacterium fortuitum group.
Image 1. Growth on 7H10 agar. Image 2. Kinyoun stain showing acid fast bacilli.
Discussion
M. fortuitum is a
group of rapid growing mycobacteria. Within the group is M. conceptionense, M. houstonense, and M. senegalense. The group
comprises the second most-commonly isolated rapidly growing mycobacterial
respiratory isolates in patients (after M.
abscessus), generally those with underlying lung disease. Progressive
pulmonary disease is generally not seen.
It has also been associated with skin and soft tissue infections
(SSTIs), surgical wound infections, lymphadenitis, and catheter-related
infections. It is seen in the environment and represents a common contaminant.
Identification is by culture and molecular techniques. It is susceptible to
many antibiotics (typically aminoglycoside, cefoxitin, imipenem, or
levofloxacin). Therapy includes two agents based on susceptibility testing for
6 to 12 months. This is somewhat controversial in pulmonary disease as the
clinical significance is not clear.
This patient is being treated through a peripheral IV. The chest
port site at two weeks showed dehiscence of the wound with drainage.
Susceptibilities are pending.
References
Park S, Suh GY, Chung MP, Kim H, Kwon OJ, Lee
KS, Lee NY, and Koh WJ. Clinical significance of Mycobacterium fortuitum isolated from respiratory specimens. Respiratory Medicine. March
2008;102(3):437-442.
Sethi S, Arora S, Gupta V, Kumar S. Cutaneous Mycobacterium fortuitum Infection:
Successfully Treated with Amikacin and Ofloxacin Combination. Indian J Dermatol.
2014;59(4):383–384.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
An 18 year old male presented to the
emergency department (ED) with fever, chills, and generalized lower abdominal
pain. He noted the fever began 6 days ago and had been intermittent since that
time. He also reported nausea and vomiting with a decrease in appetite. The
patient was from India and was treated for malaria 8 months ago, directly prior
to arrival in the United States. He stated he received three days of intravenous
medications with resolution of symptoms. In the ED, his vitals were blood
pressure 129/75, heart rate 133, temperature 104.1°F, respirations 20, and 99%
oxygen saturation on room air. On physical exam, patient had mild jaundice and
scleral icterus and severe right lower quadrant pain on palpation. CT scan of
the abdomen showed mesenteric adenitis, but no appendicitis. Initial laboratory
testing showed a mild anemia and thrombocytopenia (hemoglobin 12.1 g/dL,
hematocrit 35.9%, platelets 78,000 TH/cm2) and increased indirect
bilirubin (2.67 mg/dL). The patient received piperacillin-tazobactam while
blood and urine cultures as well as a malaria smear were pending.
Laboratory
Identification
The BinaxNOW lateral flow
immunochromatographic assay for Plasmodium
spp. was performed.
Image 1. The BinaxNOW assay was positive for malaria protein antigen, representing P. vivax, P. ovale, P. malariae, or a mix of these species.
Image 2. A thin smear showed amoeboid gametocytes in enlarged red blood cells as compared to uninfected cells (Giemsa stain, 100x oil immersion). Image 3. A thin smear showed very rare trophozoites with thick chromatin bands and single, large chromatin dots (Giemsa stain, 100x oil immersion).
The positive BinaxNOW results and
morphologic findings on smear review were most consistent with a P. vivax infection. The level of
parasitemia was approximately 0.2%. Blood and urine cultures were negative.
Discussion
Malaria classically presents with fever
and chills, weakness, headache, myalgias, nausea, and vomiting in patients who
live in tropical and subtropical regions. The four most common species that
infect humans through transmission by the female Anopheles mosquito include P.
falciparum, P. vivax, P. ovale, and P. malariae. If malaria is not diagnosed and treated in a timely
manner, complications including anemia, thrombocytopenia, renal failure, acute
respiratory distress syndrome (ARDS), and cerebral malaria can result. P. falciparum is the most deadly species
due to the parasite’s ability to cause high levels of parasitemia.
In laboratories in the United States, malaria
testing often times incorporates Plasmodium
spp. antigen detection via the BinaxNOW assay and peripheral blood smears. While
the performance of the BinaxNOW is acceptable, particularly for P. falciparum, thick and thin peripheral
blood smears remain the gold standard for malaria diagnosis, especially when
the parasitemia level is low. The thick blood smear allows for screening a
large amount of blood for malarial parasites and the thin smear allows for
species identification and assessment of parasitemia. Ideally, multiple blood
smears obtained from different times of the day should be collected in order to
exclude the diagnosis. The window prior to a febrile spike is the best time to
obtain the specimen, as the number of circulating parasites is greatest.
Clinically, the most important
distinction is between P. falciparum
and all other species. A number of features including the morphology of the
trophozoites, schizonts, and gametocytes, size of the infected red cells, the
presence of multiply infected red blood cells, and the region that the patient
lives in or traveled to are helpful in determining species level
identification.
P.
vivax infects enlarged, young red
blood cells and multiple trophozoites may be present in one red blood cell. The
trophozoites have thick, blue cytoplasm and usually one, large chromatin dot.
The schizont can contain 12 to 24 merozoites and the gametocyte is large and
oval in shape. Schuffner’s stippling and malarial pigment are common. It is important
to correctly identify P. vivax and P. ovale as they have hypnozoite forms
in the liver and patients can relapse unless they are treated with an
additional medication to eradicate these forms.
In the case of our patient, he received
chloroquine, the treatment of choice for P.
vivax arising in India. Primaquine and tafenoquine are both options for
eradication of the hypnozoite form in the liver. These medications can cause
hemolytic anemia in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiency
so quantification of the enzyme is required prior to administering therapy. Our
patient had normal G6PD levels and received tafenoquine as well.
-Karla
Perrizo, MD, is a clinical pathology resident at the University of Mississippi
Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
A 57 year old male with a recent history of a left above the
knee amputation developed a fever during the same admission of 101.1°F. His
amputation had been complicated by poor wound healing, and he had a
simultaneous right leg abscess that grew methicillin-sensitive Staphylococcus aureus. Examination of
his wound showed serosanguinous drainage with no erythema or purulence. Blood
cultures and a wound swab were sent for microbiological analysis.
Laboratory Findings
Wound cultures grew methicillin-resistant Staphyloccocus aureus thought to
represent colonization rather than true infection. Blood cultures flagged
positive in one anaerobic bottle only at 30 hours. A gram smear showed
gram-negative cocci (Image 1). Anaerobic blood plates grew pinpoint colonies
(Image 2). MALDI-TOF identified the bacteria as a Veillonella species.
Image 1. Gram stain from anaerobic culture showing gram negative cocci.Image 2. Growth on anaerobic blood plate.
Discussion
Veillonella species
are gram negative cocci. They are lactate fermenting, obligate anaerobes and
are considered normal flora of the intestines and oral mucosa. As such, they
are usually regarded as a contaminant. They have, however, been implicated in
osteomyelitis, prosthesis infections, and endocarditis. They are particularly
associated with poor oral hygiene, chronic periodontitis, and smoking. They have
important implications in dental disease due to their ability to form biofilms.
They are frequently resistant to ampicillin and have also been noted to be
resistant to tetracyclines in periodontal patients. Identification is done by
molecular methods, typically MALDI-TOF. PCR has also been developed, but is not
routinely used.
This was considered a contamination due the absence of
symptoms and isolation in one bottle only. A follow up blood culture was
negative. Routine wound care was resumed.
References
Rovery C, Etienne A, Foucault C, Berger P, Brouqui P.
Veillonella montpellierensis endocarditis. Emerg Infect Dis.
2005;11(7):1112–1114.
Mashima I, Theodorea CF, Thaweboon B, Thaweboon
S, Nakazawa F. Identification of Veillonella Species in the Tongue Biofilm by
Using a Novel One-Step Polymerase Chain Reaction Method. PLoS One. 2016;11(6):e0157516. Published 2016 Jun 21.
-Jonathan Wilcock, MD is a 1st
year anatomic and clinical pathology resident at the University of Vermont
Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
The infectious disease
service was consulted on an 83 year old male for fever.
His past medical history was significant for diabetes mellitus, anemia and renal insufficiency. He initially presented 3 weeks ago with chills, rigors and fever to 103 degrees Fahrenheit. For the past several months, the patient has had weight loss (10-20 pounds over an unspecified timeframe), fatigue and new iron deficiency anemia. A heart murmur was heard on physical exam. The patient was admitted for suspicion of sepsis and he was started on empiric antibiotics vancomycin and ceftriaxone. Three sets of blood cultures were drawn prior to initiation of antibiotics, which were all positive for gram positive cocci in pairs and chains. Transesophageal echocardiogram (TEE). TEE showed large vegetation on posterior mitral leaflet measuring 1cm x 1.8 cm, and a smaller mass on the anterior leaflet. A week after admission, a mitral valve replacement was performed followed and a portion of the valve was sent for culture (Figure 1).
Laboratory
Identification
Image 1. Gram stain from mitral valve specimen showing a large accumulation of gram positive cocci in chains (100x magnification). Image 2. Brown-Hopps stain of the surgically resected mitral valve tissue vegetation showing sheets of gram positive bacteria (40x magnification).
Discussion
The gram positive organism from blood and mitral valve culture was
identified as Streptococcus mitis by MALDI-TOF mass spectrometry. S. mitis is a member of the Streptococcus genus.
Streptococci have a number of features that aid in laboratory identification: they
are Gram positive, catalase-negative, spherical/ovoid, with organisms that are
usually found in chains. They are facultative anaerobes.
More specifically, S. mitis belongs to the viridans
streptococci group which includes Streptococcus
mutans, Streptococcus sanguis, and
Streptococcus salivarius, among many
others. The most common infection caused by viridans streptococci is bacterial
endocarditis, as in the case of this patient. Other infections can include
brain abscesses, liver abscesses, dental caries, and bacteremia.
Patients with
bacterial endocarditis have an infection of the heart valves or the endoecardial
wall that leads to formations of vegetations. These vegetations are composed of
thrombotic debris and organisms (Image 2), often associated with destruction of
cardiac tissue. Its onset often involves severe symptoms including fever,
chills, and weakness. Fever is the most consistent symptom of infective
endocarditis, but it may be subtle or even absent in some cases, especially in
older adults. Weight loss and flu-like symptoms may also be seen. Left-sided
infective endocarditis, as in the case of our patient, will present with murmur
in 90% of cases. In long-standing infective endocarditis, patients may present
with Roth spots (retinal hemorrhages), Osler nodes (subcutaneous nodules in the
digits), microthromboemboli (which appear as splinter hemorrhages under
fingernails and toenails), and Janeway lesions (red nontender lesions on the
palms or soles).
In the laboratory, the
diagnosis of S. mitis and other
viridians streptococci is often detected via blood culture as in the case
of this patient. Once the blood culture bottle becomes positive, a Gram stain is
performed, which shows Gram positive cocci in chains (Image 1). These features
are helpful in differentiating Streptococcus from Staphylococcus (which
appears as clusters instead of chains). Biochemical testing can be done to
narrow down the species and identify S. mitis, which is optochin resistant (as
opposed to S. pneumonia), acetoin negative (in contrast to most other viridans
organisms), and urease negative (which differentiates it from S. vestibularis which
is urease positive).
Surgical pathology can
also aid in diagnosis by microscopically identifying vegetations on the
affected valve (Image 2). Treatment of bacterial endocarditis is usually with
penicillin or ceftriaxone, however susceptibility testing should be performed
on S. mitis and other viridians
streptococci because resistance can occur to penicillin. Blood cultures are
followed until they are negative for 72 hours. In the case of our patient, his
cultures became negative shortly after he started treatment. Susceptibility
testing showed that the organism is sensitive to penicillin and ceftriaxone.
The patient was continued on ceftriaxone and is clinically improving.
-Haytham Hasan, MD, is
an Anatomic and Clinical Pathology resident at NorthShore Evanston Hospital
(University of Chicago).
-Erin McElvania, PhD, D(ABMM), is the Director of Clinical
Microbiology NorthShore University Health System in Evanston, Illinois.
Follow Dr. McElvania on twitter @E-McElvania.
An 8 year old male with no significant medical history
presented with left knee pain and swelling for one week. Physical examination
revealed a temperature of 101.2°F and a left swollen, tender knee with reduced
range of motion. A joint aspirate was performed, and synovial fluid and blood
were sent for microbiological analysis.
Laboratory Findings
Synovial fluid analysis showed increased neutrophils, a
nucleated cell count of 90,840 cells/cmm, and no crystals.
Blood cultures were negative. Gram smear of the joint fluid
showed many neutrophils and no bacteria. Fluid culture grew convex tan-yellow
colonies on blood and chocolate plates at 48 hours (Image 1). Gram smear
revealed gram-negative cocci (Image 2). The organism was identified by
MALDI-TOF as Aggregatibacter aphrophilus.
Antibiotic susceptibility testing showed susceptibility to augmentin,
ampicillin, ceftriaxone, and levofloxacin.
Image 1. Growth on anaerobic chocolate plate.Image 2. Gram stain from anaerobic culture showing gram negative cocci.
Discussion
Aggregatibacter
aphrophilus is a gram negative coccobacillus that requires 5% CO2 and grows
best on blood agar. It is oxidase negative and catalase negative. It is
categorized as a HACEK organism, being a cause of culture-negative
endocarditis. It is considered normal oral flora, and dental procedures can be
a source of infection. Aggregatibacter endocarditis
can cause a positive P-ANCA and be misdiagnosed as a vasculitis. It has also
been reported as causes of sacroiliitis, bartholinitis, endophthalmitis, and
brain abscesses. Treatment is generally ceftriaxone for 8 weeks. Identification
is by biochemical methods or MALDI-TOF. Broad range PCR (br-PCR) has also been
described, which targets a highly-conserved region of 16S rDNA, and then
compares the sequences to database sequences.
The patient was given cefazolin, and his temperature
downtrended. He was discharged prior to results but placed on oral augmentin.
After susceptibility testing, infectious disease was consulted and he was
placed on ceftriaxone for 8 weeks. He continued to improve and subsequent
cultures were negative.
References
Ratnayake L, Olver WJ, Fardon T. Aggregatibacter
aphrophilus in a patient with recurrent empyema: a case report. J Med Case Rep.
2011;5:448. Published 2011 Sep 12. doi:10.1186/1752-1947-5-448
Hirano K, Tokui T, Inagaki M, Fujii T, Maze Y,
Toyoshima H. Aggregatibacter aphrophilus infective endocarditis confirmed by
broad-range PCR diagnosis: A case report. Int J Surg Case Rep. 2017;31:150–153.
doi:10.1016/j.ijscr.2017.01.041
-Jonathan Wilcock, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology
at the University of Vermont Medical Center and an Associate Professor
at the University of Vermont.
A 58 year old female with no significant past medical history presented her primary care physician with chief complaint of abdominal pain. She reported continued vague abdominal symptoms for the past two months, with intermittent diarrhea and increased flatulence. No recent travel history or significant exposures were identified. An ultrasound of the right upper quadrant was unremarkable and no gallstones were present. The patient was scheduled for a screening colonoscopy. A stool specimen was submitted to the microbiology laboratory for stool culture and ova & parasite exam.
Laboratory
Identification
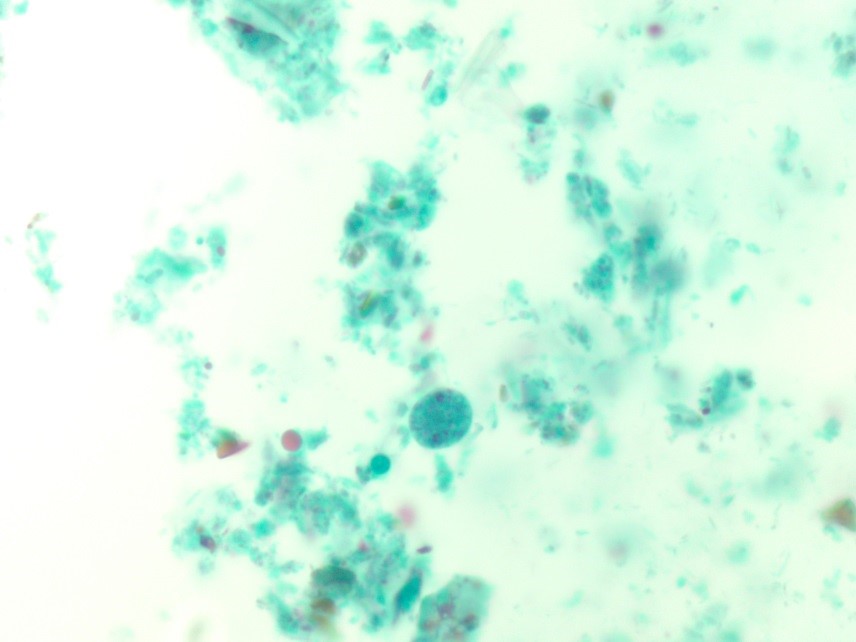
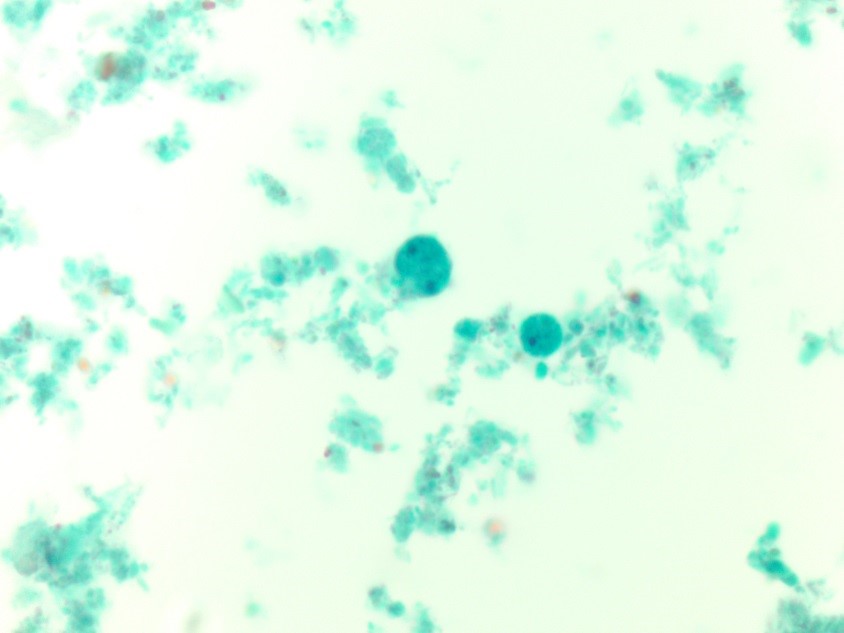
Image 1. Trichrome stained fecal smear illustrating a binucleated trophozoite with fragmented karyosomal material from a stool ova & parasite exam. Image 2. Additional trichrome fecal smear image highlighting both uninucleate and binucleate trophozoites that range in size from 5 to 15 um.
The findings from the ova and parasite
exam were consistent with Dientamoeba
fragilis, an intestinal flagellate. The stool culture was negative for Salmonella, Shigella, and Escherichia coli 0157:H7.
Stool enzyme immunoassays were negative for Campylobacter
spp.and Shiga toxin 1 and 2.
Discussion
Dientamoeba
fragilis is an intestinal flagellate
with worldwide distribution and causes asymptomatic and symptomatic infections,
predominantly in small children. Symptoms of infection may include intermittent
diarrhea, abdominal pain, anorexia, weight loss, and flatulence. While the pathogenesis is not completely
understood, transmission is thought to occur via the fecal oral route and it is
hypothesized that the trophozoites are transmitted via the eggs of nematodes, Enterobiusvermicularis and Ascaris
lumbricoides, due to a higher incidence of co-infections between these
organisms than expected.
In the laboratory, the diagnosis of D. fragilis is made by ova and parasite
exam. The trophozoite resembles amebae and is typically 9-12 µm. Most
trophozoites are binucleate with finely granular cytoplasm and the within the nuclei
there are 4-8 fragments of karyosomal granules (Figure 1). Due to the fact that
30-40% of D. fragilis trophozoites
are uninucleate (Figure 2) and they lack external flagella, they must be
differentiated from Endolimax nana and
Entamoeba hartmanni, which are both
non-pathogenic amebae. Historically, no cyst phase was known for D. fragilis; however, recent studies have
identified precyst forms or putative cysts. Permanently trichrome stained
slides are essential to diagnosing D.
fragilis infection, as the organism is hard to detect in concentrated
smears.
Since our patient was symptomatic, she was treated with iodoquinol, the drug of choice for D. fragilis infections. Her symptoms resolved and colonoscopy did not reveal additional pathology.
-Debbie Walley, MD, is a 4th year Anatomic and Clinical Pathology chief resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.
A 15 year old male with a past medical history significant
for Tetralogy of Fallot (congenital heart defect), multiple valve replacements,
chronic kidney disease, and prior Bartonella endocarditis. He presented with a
“flu-like” illness including muscle aches, fevers, fatigue, and night sweats. His
symptoms slowly dissipated after about three days. However, he had labs drawn
including multiple blood culture sets which were all positive for growth.
Laboratory Findings
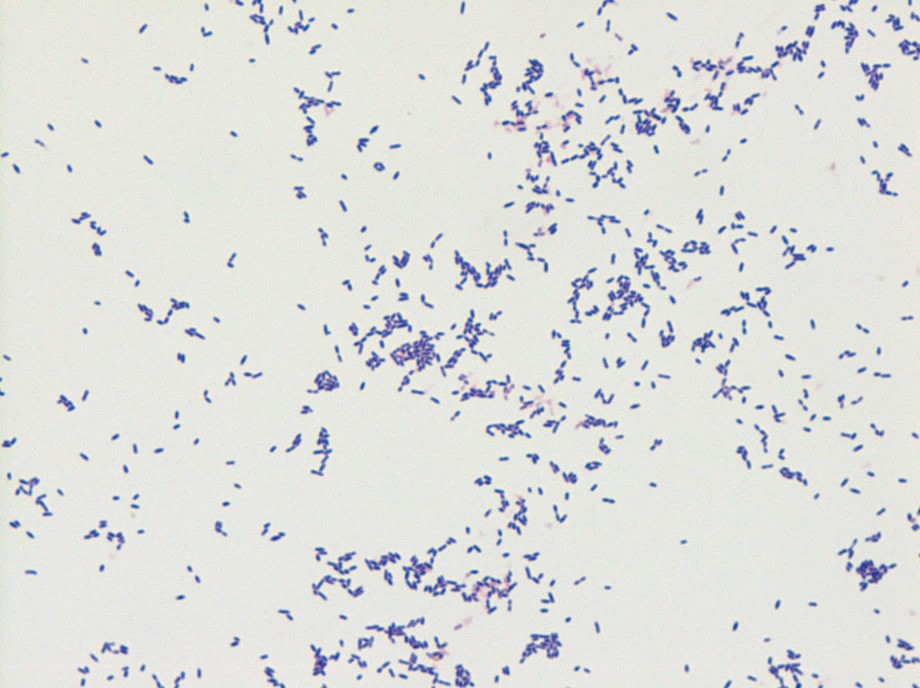
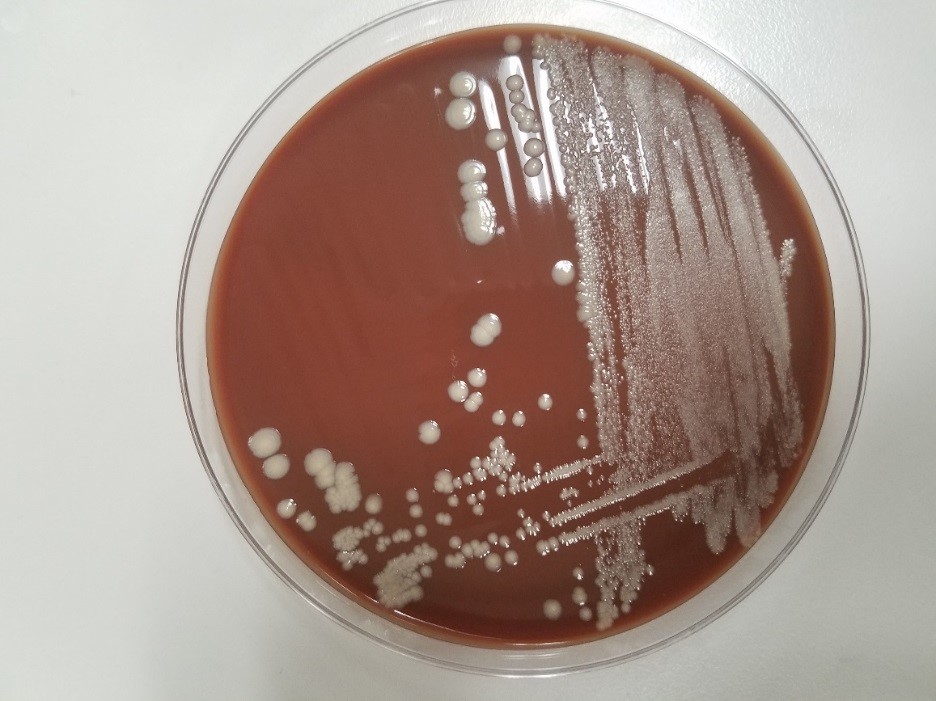
Gram stain showed gram positive bacilli and culture plates grew two morphologies of slow growing gray, granular and opaque colonies.This organism was identified by MALDI-TOF as Corynebacterium pseudodiphtheriticum.
Image 1. Gram stain with gram positive bacilli .Image 2. Culture with small, grayish colonies with granular appearance and opaque centers (growth at day 2).
Discussion
The
genus Corynebacterium comprises a
collection of irregular-formed, rod-shaped or coccoid bacteria that are
non-motile, catalase-positive, and non-spore-forming.
Corynebacterium
pseudodiphtheriticum
(previously designated as Corynebacterium
hofmannii) is a nonlipophilic, nonfermentive, urease- and nitrate-positive Corynebacterium species.1C. pseudodiphtheriticum is part of the
usual oropharyngeal bacterial flora, including the nares and throat. It appears
to play a role in preventing colonization of oropharyngeal epithelia by
pathogenic bacteria.
Most
commonly, C. pseduodiptheriticum is a
pathogen of the respiratory tract with cases of nosocomial and
community-acquired pneumonia, bronchitis, tracheitis, pharyngitis, and
rhinosinusitis. Endocarditis is the second most common infection site, although
very rare. Cases of urinary tract and wound infections have also been reported.
Treatment
is usually with penicillin alone or in combination with aminoglycosides. Antibiotic
susceptibility profiling of C.
pseudodiphtheriticum isolates showed that resistance to oxacillin,
erythromycin, clindamycin, and macrolides are common.1
-Nicole Mendelson, MD
is a 1st year Anatomic and Clinical Pathology resident at the
University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 24 year old male with no past medical history presented with
fevers, myalgia, and cough following return from a 1-week trip to Guatemala
where he spent significant time within caves. The patient described his cough
as persistent, non-productive, and associated with mild shortness of breath at
rest that significantly worsens with activity. In the emergency department, the
patient was afebrile with a WBC of 10.2, Transaminitis, and chest X-ray showed
diffuse reticular pattern. He underwent a bronchoscopy and BAL washout.
Laboratory Findings
Histoplasmosis Urine Antigen test came back positive.
Image 1. Fungal culture with white/tan, fluffy mold (growth at day 7).Image 2. Scotch tape prep with tuberculate macroconidium. This mold was morphologically identified as Histoplasma capsulatum and sent to Mayo Laboratories for further confirmatory testing.
Discussion
Histoplasma
capsulatum is an intracellular, thermally dimorphic fungus (grows as a
yeast at body temperature/37°C in humans or culture media and as mold at 25°C
in the environment/culture media). Histoplasma
is found in soil, particularly in areas containing bird and bat droppings,
such as caves. Within the United States Histoplasma
in found in central and eastern states with a predominance in the Ohio and
Mississippi River Valleys. This fungus is also found in parts of Central and
South America, Africa, Asia, and Australia.
Infection with
Histoplasma capsulatum causes
significant morbidity and mortality worldwide. Upon inhalation of conidia, H. capsulatum transforms into the
pathogenic yeast phase. This form replicates within macrophages that carry the
yeast from the lungs to other organs. Histoplasmosis has three main forms:
Acute
primary histoplasmosis which presents as a pneumonia with fever, cough,
myalgia.
Chronic
cavitary histoplasmosis which is characterized by pulmonary lesions that often
resemble cavitary tuberculosis.
Progressive
disseminated histoplamosis that spreads to infect many organs in
immunocomprimised patients.
In the laboratory, culture of blood, tissue and respiratory
specimens may be completed. In addition, a test for H. capsulatum
antigen is sensitive and specific when simultaneous serum and urine specimens
are tested. It is important to note that cross-reactivity with other fungi (Coccidioides
immitis, Blastomyces dermatitidis, Paracoccidioides brasiliensis,
Penicillium marneffei) has been identified.
Growth on fungal culture shows white/tan, fluffy mold
that turns to brown to buff with age. The organism may also produce wrinkled,
moist, or heaped yeast-like colonies that are soft and cream when grown at 37°C
on certain media. Scotch tape preparation of the mold form shows tuberculate
macroconidia, a diagnostic structure of Histoplasma
capsulatum. The mycelia are septate and produce microconidia and
macroconidia. Yeast forms of Histoplasma
capsulatum are small (2 to 4 μm) and reproduce by budding. These budding
forms may be seen on histology specimens. A commercially available DNA probe
can be performed on culture material to confirm identification.
Patients with mild-moderate histoplasmosis can often have
resolution of their symptoms without treatment. Those with more moderate-severe
disease require antifungal agents including amphotericin B or itraconazole.
-Nicole Mendelson, MD
is a 1st year Anatomic and Clinical Pathology resident at the
University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
A 30 year old
African American male presented to the emergency department (ED) with fevers
and cough. His past medical history was significant for type 1 diabetes & diabetic
nephropathy requiring a kidney/pancreas transplant
three years prior. He is compliant with his immunosuppressant regimen. He
described the cough as non-productive and denied shortness of breath or chest
pain. He denied sick contacts, recent travel, and has no pets. After hospital
admission, he became septic, developed severe hypotension (70/30s), and was transferred to the
intensive care unit (ICU). Chest x-ray showed multifocal consolidations in
bilateral lung fields and a small pleural effusion consistent with pneumonia. He was empirically started
on vancomycin, piperacillin-tazobactam, azithromycin, and micafungin.
Infectious diseases was consulted and recommended a board variety of tests and
cultures given the patient immunosuppressed status.
Laboratory Identification
The following
results were obtained:
Sputum
culture: normal respiratory flora, negative for fungi and acid fast bacilli
Respiratory
viral PCR panel: positive for adenovirus, coronavirus, and rhinovirus
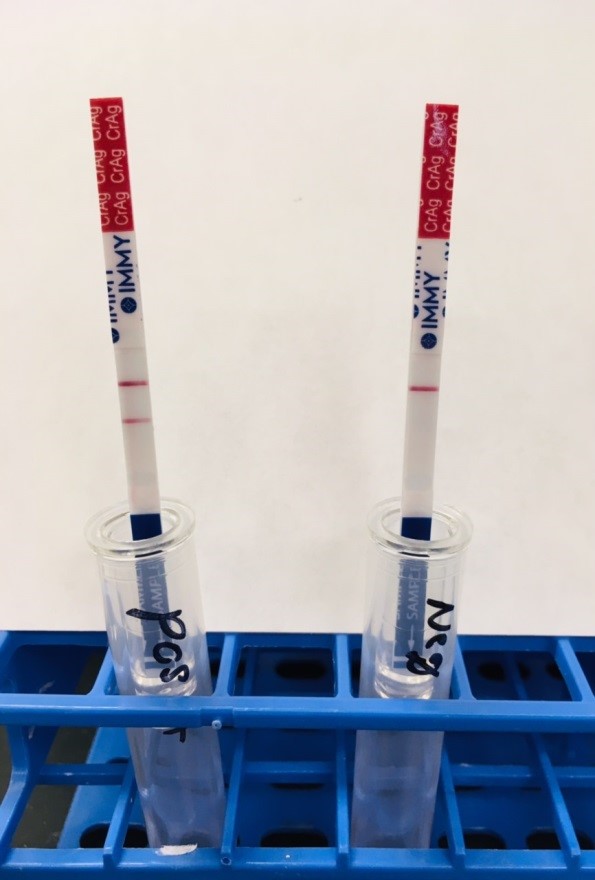
Image 1. Cryptococcal lateral flow assay showing positive (left) and negative (right) results. The patient had a positive result from the serum with a titer of 1:20.
Given this positive serum result for Cryptococcus neoformans despite multiple negative sputum cultures, a bronchoalveolar lavage & lumbar puncture were performed and bacterial & fungal cultures were performed.
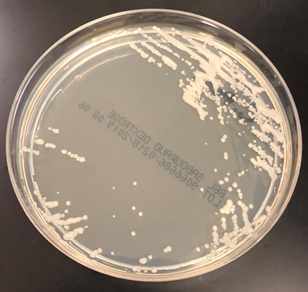
Image 2. Discrete, mucoid, cream colored colonies of Cryptococcus neoformans growing on Sabouraud dextrose agar after the third week of incubation at 25°C from the bronchoalveolar lavage specimen.
Discussion
Cryptococcus neoformans is an encapsulated yeast that
is most commonly acquired through inhalation and can infect & disseminate
to multiple organ systems including the lungs, central nervous system, skin and
bones, especially in immunocompromised patients such as those with HIV or organ
transplant patients. The thick polysaccharide capsule gives colonies of C. neoformans a mucoid appearance, serves
as a major virulence factor, and also plays an important part in various
laboratory identification methods.
In the lab, C. neoformans will grow a variety of
selective and non-selective agars including blood, chocolate, Sabouraud dextrose,
and cornmeal agars as discrete, cream colored colonies (Image 2). On
microscopic examination, the C.
neoformans yeast are gram positive with narrow based budding and a thick
capsule. The yeast vary in size from 2-20 µm and are evenly spaced from one
another due to the capsule. C. neoformans
is positive for both urease and phenoloxidase. Historically, India ink stain
was performed on CSF specimens to highlight the capsule using direct
microscopy. Grocott’s methenamine silver (GMS), mucicarmine, and Fontana-Masson
histochemical stains are all positive for C.
neoformans.
Cryptococcal
antigen tests directed to the capsular polysaccharide can also be used to
diagnosis C. neoformans infections
from both serum and CSF specimens. Common methods include immunochromatographic
lateral flow assays or particle agglutination. Advantages to these methods
include increased sensitivity and the ability to provide semi-quantitative
titer results which can be used to monitor the patient’s response to therapy.
Rarely, false negative results can occur due to extremely high concentrations
of the cryptococcal antigen. In order to combat the prozone effect, the sample
should be diluted prior to repeating the test if there is a high suspicion of
cryptococcal infection. False positive results may also occur when macroglobulins
are present in the sample due to disease states such as rheumatoid arthritis or
lupus. Use of pronase can prevent the interference of macroglobulins on serum
test results. False positive test results have also be documented due to interferences
from various collection devices such as anaerobic vials.
In the case
of our patient, as C. neoformans is
intrinsically resistant to echinocandins, he was switched from micafungin to
fluconazole. He responded well and after completing the therapeutic course, he
continued on a prophylactic dose of fluconazole. His cerebrospinal fluid
culture showed no growth and the cryptococcal lateral flow assay was negative
on the CSF specimen.
-Charles Middleton, MD, is a first year Anatomic and Clinical
Pathology resident at the University of Mississippi Medical Center.
-Lisa Stempak, MD, is an Assistant Professor of Pathology at the
University of Mississippi Medical Center in Jackson, MS. She is
certified by the American Board of Pathology in Anatomic and Clinical
Pathology as well as Medical Microbiology. She is the Director of
Clinical Pathology as well as the Microbiology and Serology
Laboratories. Her interests include infectious disease histology,
process and quality improvement, and resident education.