A worm specimen—as shown in Image 1—was found in a stool sample from a 21 month old, otherwise healthy female.
Image 1. Specimen collect from patient’s stool.
Discussion
The worm specimen in question is Ascaris lumbricoides, the largest of the nematode parasites. Females typically measure 20-35 cm long with straight tails, while males are smaller at 15-31 cm with curved tail.1 A characteristic feature in adults of both sexes are the three “lips” at the anterior end of the body, as shown in Image 2.
Image 2. Close up of the anterior end of an adult A. lumbricoides. Three “lips” are highlighted with a black arrow.
Humans are the definitive host for these roundworm parasites. Infection with these soil-transmitted helminths is quite common, with an estimated 807 million to 1.2 billion people affected.2,3 Children are infected much more frequently than adults.4 Nearly all A. lumbricoides cases occur in tropical and subtropical areas of Asia, sub-Saharan Africa, and the Americas. This infection is rare or absent in developed countries, but sporadic cases may occur in rural regions.3
Individuals affected with adult Ascariasis worms usually show no acute symptoms. However, since these worms are commonly situated in the small intestines, the clinical presentation of a heavy worm burden in children might include stunted growth via malnutrition. In both adults and children, a high worm burden may result in abdominal pain and intestinal obstruction leading to potential perforations. Migrating worms may lead to symptomatic occlusion of the biliary tract, appendicitis, or nasopharyngeal expulsion.3
In the clinical setting and for diagnosis, A. lumbricoides eggs should be found in the feces, juvenile worms in the sputum, and in some cases adults in the feces. For deworming, the recommended treatment are anti-helminthic medications such as albendazole and mebendazole.3 These medications kill the adults, but not the migrating larvae thus repeat treatment might be needed.
References
Centers for Disease Control and Prevention. DPDx – Laboratory Identification of Parasites of Public Health Concern. Internet [updated July 19, 2019]. Available from: https://www.cdc.gov/dpdx/ascariasis/index.html.
Veesenmeyer AF. Important Nematodes in Children. Pediatr Clin North Am. 2022;69(1):129-39. Epub 2021/11/20. doi: 10.1016/j.pcl.2021.08.005. PubMed PMID: 34794670.
-Amelia Lamberty is a Masters Student in the Department of Pathology and Laboratory Medicine at the University of Vermont.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont
A middle-aged female presented to the emergency department after experiencing a fall and loss of consciousness due to syncope. Upon presentation, the patient endorsed an almost four-week history of fevers, chills, abdominal discomfort, night sweats, and dizziness. She also reported poor oral intake and recent unintended weight loss since the onset of her symptoms. When asked, she noted she had returned from a month-long trip to Italy and Ghana two months prior to presentation. She initially presented to an outside hospital with generalized weakness, body aches, and a fever where she was treated with antibiotics for a urinary tract infection. She then presented to a different outside hospital with similar symptoms. There, she confirmed she had not taken malaria prophylaxis and was bitten by mosquitos on her recent trip. Blood was taken for a peripheral blood smear review but no Plasmodium sp. were observed.
At her current presentation, the patient denied a history of seizures but continued to endorse recurrent fevers, malaise, nausea, and vomiting. She was mildly tachycardic, afebrile, and bloodwork revealed normocytic anemia (hemoglobin 10.3), and elevated creatinine. Given the uncertainty surrounding her syncopal episode, the patient was admitted for further workup. After admission, she spiked a fever up to 103°F and the infectious disease service was consulted. As part of her workup, blood was again drawn for Giemsa-stained peripheral blood smears which were read in the microbiology laboratory.
Laboratory Identification
Upon receipt of the patient’s blood, Giemsa-stained thick and thin smears and an immunochromatographic assay for the detection of malarial antigens (BinaxNOW® Malaria, Abbott Laboratories, Abbott Park, IL) were performed. The BinaxNOW® assay was positive for the detection of pan-malarial antigen (T2), but not the histidine-rich protein II antigen specific to P. falciparum (T1). These findings were suggestive of infection with a non-falciparum Plasmodium species (Image 1). Analysis of the Giemsa-stained thin smear revealed several Plasmodium parasites at various stages of development. Importantly, parasites (and particularly ring forms) were only rarely encountered (Image 2, Image 3A). “Basket” (Image 3B) and “Band” (Image 3C) trophozoite forms were observed, as well as schizonts with 6-12 merozoites typical rosette patterns around central pigment (Image 3D). In the context of a positive antigen test, the patient was definitively diagnosed with a Plasmodium malariae infection based on morphology with a calculated parasitemia of less than 0.1%.
Image 1. BinaxNOW® Malaria assay. This patient’s assay was positive for the common malarial antigen (T2), but the histidine-rich protein II antigen (T1) specific to P. falciparum was not detected. These results suggest an infection with a non-falciparum Plasmodium species.Image 2. Developing ring-form trophozoites of P. malariae. Ring form trophozoites of P. malariae are less-frequently encountered in peripheral smears compared to other Plasmodium species that infect humans. A) P. malariae rings usually have a single chromatin dot and are generally thicker than that of P. falciparum. B) As rings develop, the cytoplasm can extend across the cell or can appear with vacuolation leading to “band” or “basket” forms, respectively.Image 3. Gimesa-stained thin smear of erythrocytes infected with P. malariae. A) CellaVision® field with rare infected erythrocytes notated by black arrowheads. B) “Basket” form trophozoite of P. malariae. C) “Band” trophozoite of P. malariae. D) Schizont of P. malariae with 6-12 merozoites surrounding central pigment in a characteristic “rosette”.
Discussion
Plasmodium malariae is one of the five species of Plasmodium (along with P. falciparum, P. vivax, P. ovale and P. knowlesi) which cause human malaria. Infection begins when sporozoites are injected from the salivary glands of the female Anopheles mosquito into the host upon taking a blood meal. Sporozoites migrate to the liver where they infect hepatocytes and develop into schizonts which eventually rupture, releasing infectious merozoites. These merozoites enter the circulation and infect erythrocytes, subsequently developing into immature ring form trophozoites (Image 2A). Ring form trophozoites develop into either mature trophozoites or become gametocytes which can be taken up by another mosquito upon feeding (Image 2B). Mature P. malariae trophozoites adopt unique morphologies not seen with other Plasmodium species including “band” (Image 3B) and “basket” (Image 3C) forms. Mature trophozoites then develop into schizonts (Image 3D) which rupture, releasing 6-12 merozoites which perpetuate the erythrocytic cycle of infection. P. malariae elaborates fewer merozoites than other Plasmodium species which are often arranged in a “rosette” pattern around centrally localized pigment in the schizont (Image 3D).
The P. malariae infectious cycle has several unique hallmarks compared to that of other Plasmodium species. Unlike P. vivax and P. ovale, the P. malariae lifecycle does not include a latent hypnozoite form, and thus is devoid of classical relapse. P. malariae also preferentially infects older erythrocytes, as opposed to P. vivax which prefers younger cells. Additionally, the infected erythrocyte does not enlarge or fimbriate when infected with P. malariae as opposed to P. vivax and P. ovale, respectively. Patterns of erythrocyte infection and lysis lead to elevated parasite burden, characteristic cyclic fevers and anemia. However, the time needed for development from ring trophozoite to rupturing schizont is different among malarial parasites: P. knowlesi exhibits the most rapid development (24-hours), followed by P. falciparum, P. ovale, and P. vivax (48-hours), and then P. malariae (72-hours).
P. malariae has a global distribution overlapping with P. falciparum. While P. falciparum is the primary species causing reported infection in Ghana, P. malariae infection is encountered less frequently. Associated parasitemia are characteristically lower in P. malariae infections compared to other species due to fewer merozoites produced during infection, an extended 72-hour developmental cycle, and the preference for the infection of older erythrocytes. This can complicate microscopic diagnosis as well as lead to more indolent symptomology. Indeed, patients can often remain asymptomatic for months to years after leaving endemic areas. In this patient’s case, definitive diagnosis was made months following her travel to an endemic region. The patient completed a 5-day course of artemether/lumefantrine with complete resolution of symptoms prior to discharge.
-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
A preteen boy presented to primary care office with a complaint of flu-like symptoms for the past five weeks. His symptoms improved after 2-3 weeks but noted acute worsening of symptoms in the last two weeks, including sore throat, head congestion, and cough. The physical exam was unremarkable except for nasal congestion, mucosal edema, and some drainage. A chest X-ray was taken, which was normal. Results were negative for a Streptococcal infection, SARS-CoV-2, Bordetella pertussis, and influenza. Bordetella parapertussis was detected by PCR (Image 1).
Image 1. Bordetella pertussis and Bordetella parapertussis PCR. Green = IS481, target gene for B. pertussis. Red = IS1001, target gene for B. parapertussis. Purple = Internal control (IC)
Discussion
Bordetella is a small, non-fermentative, gram negative coccobacilli. The genus Bordetella has 15 species, and B. pertussis & B. parapertussis are most commonly found in human infections causing pertussis. B. parapertussis usually cause milder disease, but reports of outbreaks of B. parapertussis have increased in recent literature. The epidemic cycles for pertussis occur at 3–4 years intervals2 and pertussis vaccination does not prevent B. parapertussis infection. B. parapertussis generally occurs in a younger age group than disease caused by B. pertussis.4 Cherry et al. indicated that B. parapertussis infections contribute significantly to the disease burden, which was previously thought to be vaccine failure in children.2
Pertussis is primarily a toxin-mediated disease; the bacteria attach to the cilia of the respiratory epithelial cells and produce toxins that paralyze the cilia and cause inflammation of the respiratory tract, which interferes with the clearing of pulmonary secretions.1B. pertussis and B. parapertussis are almost identical at the DNA level and produce many similar virulence factors like as filamentous hemagglutinin (FHA), pertactin, tracheal cytotoxin, dermonecrotic toxin, and adenylate cyclase-hemolysin. An essential difference between the two is that B. parapertussis does not secrete pertussis toxin.3,5-9 Despite the high degree of homology shown by the amino acid sequences of the main antigens, the two species differ in respect to several protective epitopes.10
Pertussis (whooping cough) can cause serious illness in babies. Symptoms of pertussis usually develop within 5-10 days of exposure. Early non-specific symptoms, including runny nose, low-grade fever, and occasional cough, can last for 1 to 2 weeks. After 1 to 2 weeks, as the disease progresses, paroxysms occur, which are many, rapid coughs followed by a high-pitched “whoop” sound. Vomiting or exhaustion develops at this stage. Recovery from pertussis is slow, the cough becomes milder and less common, but coughing fits can return with other respiratory infections for many months after the pertussis infection started. The “whoop” is often absent or mild in less severe disease. The illness is generally milder in teens and adults, especially those who have gotten the pertussis vaccine. The cough can be minimal or absent in babies, but they might get apnea, which is most dangerous.1
Bordetella is a fastidious organism as it requires special media, prolonged incubation, timely transport, and rapid plating for recovery of the organism. Regan low and Bordet Gengou are the special media used for culture of B. parapertussis and B. pertussis. Unlike B. pertussis, B. parapertussis can grow on blood and chocolate agar. Colonies may appear like mercury drop and produce beta hemolysis on prolonged incubation. Culture has the highest recovery if a nasopharyngeal swab is collected within two weeks of symptom onset. Sensitivity can be as high as 56% in early disease and decrease over time, while specificity is 100%.1 Serological assay are not clinically validated and do not help differentiate between recent or remote infection or vaccination. PCR is the most sensitive methodology and should be performed from a nasopharyngeal swab taken within three weeks of symptom onset; after the fourth week of cough, the amount of bacterial DNA rapidly diminishes, which increases the risk of obtaining falsely-negative results. PCR-detectable B. pertussis DNA in some pertussis vaccines and the contamination of the clinic environment by those vaccines increases the risk of false-positive PCR. As per CDC guidelines, PCR in asymptomatic persons, asymptomatic close contacts of a confirmed case, and after five days of antibiotic use is unlikely to benefit and is generally not recommended because of the risk of false positivity. In our lab, we use the DiaSorin Simplexa Bordetella direct assay system – RT PCR which targets IS481 and IS1001 for pertussis PCR (other PCR may use different targets). B. pertussis contains ∼238 copies of IS481 and no copies of IS1001, multiple copies of IS481 are responsible for the high sensitivity of PCR and increased risk of false-positive. B. parapertussis has ∼22 copies of IS1001 and no copies of IS481; false-positive identification of IS1001 seems unlikely, as IS1001 is not present in vaccines and its copy numbers are low.2
The recommended antimicrobial agents for treatment or chemoprophylaxis is azithromycin. Antibiotic susceptibility data indicate that the same antibiotics recommended for treating and preventing B. pertussis might help treat and prevent B. parapertussis.11,12 CDC recommends vaccinating young children, preteens, pregnant women, and adults, but pertussis vaccine immunity is short-lived and wanes after 7- 10 years. Immunized children become susceptible after that and can transmit B. pertussis to their very young infant siblings or get B. parapertussis as the vaccine does not protect against it. The average age of patients with B. parapertussis is much younger than those with B. pertussis, and some literature suggest B. parapertussis should be considered when developing new pertussis vaccines.13
Blom J., Hansen G. A., and Poulsen F. M.Morphology of cells and hemagglutinogens of Bordetella species: resolution of substructural units in fimbriae of Bordetella pertussis.Infect. Immun.421983308317 Crossref. PubMed.
Cookson B. T. and Goldman W. E.Tracheal cytotoxin: a conserved virulence determinant of all Bordetella species.J. Cell. Biochem.11B1987124
Endoh M., Takezawa T., and Nakase Y.Adenylate cyclase activity of Bordetella organisms. Its production in liquid medium.Microbiol. Immunol.24198095104 PubMed.
Li L. J., Dougan P., Novotny P., and Charles I. G.P70 pertactin, an outer membrane protein from Bordetella parapertussis: cloning, nucleotide sequence and surface expression in Escherichia coli.Mol. Microbiol.51991409417 PubMed.
Mooi F. R., van der Heide H. G. J., TerAvest A. R., Welinder K. G., Livey I., van der Zeisj B. M. A., and Gaastra W.Characterization of fimbrial subunits from Bordetella species.Microb. Pathog.3198718 PubMed.
He Q, Viljanen MK, Arvilommi H, Aittanen B, Mertsola J. Whooping Cough Caused by Bordetella pertussis and Bordetella parapertussis in an Immunized Population. JAMA. 1998;280(7):635–637. doi:10.1001/jama.280.7.635
Hoppe JE, Bryskier A. In vitro susceptibilities of Bordetella pertussis and Bordetella parapertussis to two ketolides (HMR 3004 and HMR 3647), four macrolides (azithromycin, clarithromycin, erythromycin A, and roxithromycin), and two ansamycins (rifampin and rifapentine). Antimicrob Agents Chemother. 1998 Apr;42(4):965-6. doi: 10.1128/AAC.42.4.965. PMID: 9559823; PMCID: PMC105582.
Mortensen JE, Rodgers GL. In vitro activity of gemifloxacin and other antimicrobial agents against isolates of Bordetella pertussis and Bordetella parapertussis. J Antimicrob Chemother. 2000 Apr;45 Suppl 1:47-9. doi: 10.1093/jac/45.suppl_3.47. PMID: 10824032
Karalius VP, Rucinski SL, Mandrekar JN, Patel R. Bordetella parapertussis outbreak in Southeastern Minnesota and the United States, 2014. Medicine (Baltimore). 2017 May;96(20):e6730. doi: 10.1097/MD.0000000000006730. PMID: 28514288; PMCID: PMC5440125.
Karalius VP, Rucinski SL, Mandrekar JN, Patel R. Bordetella parapertussis outbreak in Southeastern Minnesota and the United States, 2014. Medicine (Baltimore). 2017 May;96(20):e6730. doi: 10.1097/MD.0000000000006730. PMID: 28514288; PMCID: PMC5440125.
-Payu Raval, MD is a 1st year anatomic and clinical pathology resident at University of Chicago (NorthShore). Her academic interests include hematology, molecular, and surgical pathology.
-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
In many laboratories, managing safety is rarely a full- time job. Many have to oversee the safety program while also managing day-to-day operations, and overseeing the quality or point of care programs. Some are lucky enough to be able to spend all of their time on the lab safety program. Either way, the role can include managing safety policies and procedures, performing audits, providing education and training, and consistently working to improve the overall culture.
But what happens when the lab safety officer has a job change, a promotion or is ready for retirement? What happens to all of that safety knowledge and experience? Wouldn’t a gap like that be a detriment to the lab’s safety program? Yes, and laboratories should always be preparing for such an event.
One way to get prepared for a transition of lab safety duties is to identify a potential replacement while you are still working in your role. Look for someone who has shown interest in your work or has asked good questions about safety issues. Ask them to shadow you as you perform your safety tasks. Ask them to review safety procedures that are due to be revised. Have them watch a lab safety audit and describe how it should be performed. Ask them to create and possibly present safety education for the staff.
This may seem more difficult if you are the lab manager with safety responsibilities. However, there can be a benefit to identifying someone among the staff to perform some of the safety tasks as they can eventually come off of your plate. Leaders should also always have an active succession plan, so if safety must remain under your purview, make sure it is part of your discussions with your potential leadership replacement(s).
If, as a safety leader you run a laboratory safety committee, look for potential future safety leaders in that group. There may be one or more good candidates for future lab safety leadership. You can assess their readiness by delegating projects and tasks. Again, things like creating safety education, working on policies, and performing audits are great “auditions” for a future job. You can also ask the committee to create a safety fair, or to develop a safety poster contest or other projects which help to raise safety awareness in the department.
Provide resources for potential leaders such as safety documents and regulations. Involve them in lab safety inspections. If the EPA, the local fire department, or even the wastewater authority arrives for an audit, allow those staff members to be involved in the process. Getting a taste of these typical lab safety events can help people discern whether or not they want a future in the field. Preparing the lab for an upcoming accreditation inspection is also great experience.
Another way to help someone on their path if they are interested in safety is to help them get certified. ASCP offers a Qualification in Lab Safety (QLS). Preparing for the certification will help someone learn more about specific safety topics like Bloodborne Pathogens, Chemical Hygiene, and Waste Management among others. The suggested study resources and references will remain important in the hands of a future lab safety leader.
Given the growing shortage of laboratorians, it is clear that it will become more difficult to fill job openings as the years pass. Labs cannot operate without specific people, however. Leaders are vital, bench staff are key, and safety professionals will always be necessary. Planning for succession is something that should be inherent in the department for most positions. The organizational chart should be designed with succession in mind and a staffing plan that goes beyond today. Lab Safety should always be a key piece in the lab’s overall succession process.
–Dan Scungio, MT(ASCP), SLS, CQA (ASQ) has over 25 years experience as a certified medical technologist. Today he is the Laboratory Safety Officer for Sentara Healthcare, a system of seven hospitals and over 20 laboratories and draw sites in the Tidewater area of Virginia. He is also known as Dan the Lab Safety Man, a lab safety consultant, educator, and trainer.
Preface: I wish we lived in a world where cancer did not exist. While I do not foresee that being a reality in my lifetime, I hope I can witness a milestone in oncology when the development of safe and effective therapies surpasses the rate of metastasis. I hope to see the day when instead of being five steps behind cancer, we gain our footing and come out at least one step ahead. We can’t be that far away, right? When I see a patient who is younger than me or around my age, I can’t help but ask myself, “why they have to go through this? Why do they have to be diagnosed with cancer?” Now, they have to choose whether or not to undergo fertility sparing treatment in addition to making a shared decision regarding cytotoxic therapy and radiation. They’re just beginning their life, their career, their family; they’re finally building their story, and it’s interrupted by cancer. Rather than a partner or friend, I see many younger patients present to our clinic with a parent. Imagine how that feels to be a parent – knowing your child was just diagnosed with a terminal disease. How does one cope with that? No parent should have to endure the pain and emotional suffering of losing their child to cancer, let alone anything. We’re meant to outlive our parents, we’re meant to enjoy a full and healthy life, and this case tore right through me.
The patient, a 28 year old male, first presented to an out-of-state health system after managing intermittent right hip discomfort with NSAIDs and ice for three years. When the pain worsened, he went to an urgent care toward the end of 2018, but his X-rays were negative. After his pain became unbearable six months later, he had an MRI which demonstrated a proximal femur lesion with hip and sacral involvement. The femoral lesion biopsied via FNA, and the patient underwent 6 cycles of induction chemotherapy prior to resection. The patient’s PET scan showed improvement, and the 10.5 cm hip mass was resected demonstrating fibrosis and no residual disease. Additional chemotherapy was prescribed for consolidation followed by radiation to the sacral lesions. Seven months after no evidence of disease, a surveillance PET scan demonstrated abundant bone lesions in the arms, ribs, and pelvis. A new relapse chemotherapy regimen was prescribed for refractory disease, but within cycle 2, new calvarial lesions were identified. By the beginning of 2021, the patient underwent stem cell harvesting followed by myeloablative/salvage chemotherapy and an autologous stem cell transplant. Soon after he transferred his care to our institution a few months later, the patient underwent a successful stem cell transplant and remained stable for three months post-transplant. The patient began experiencing severe pain which prompted earlier surveillance imaging, and both PET scan and MRI demonstrated extensive disease progression. To improve comfort and confirm etiology, a right thoracentesis was performed, and 1,200 mL’s of bloody fluid was sent to our cytology lab for analysis. The findings are presented below.
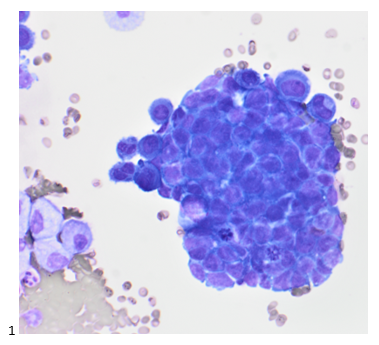
At our institution, we use one or two drops of fresh fluid to make a cytospin for triage purposes. We examine the air-dried, Diff-Quik-stained cytospin to determine whether or not the cells are likely to contaminate our routine preparations, and if the cells are overtly malignant, the remaining cytopreparations need to be stained in our known-positive fluid set-up. In this case, the specimen was deemed routine despite the few clusters of cells that do not resemble the predominating mesothelial cells. The tightly clustered group in Image 1 has small, round nuclei; fine chromatin; scant, blue cytoplasm; and atypical mitoses.
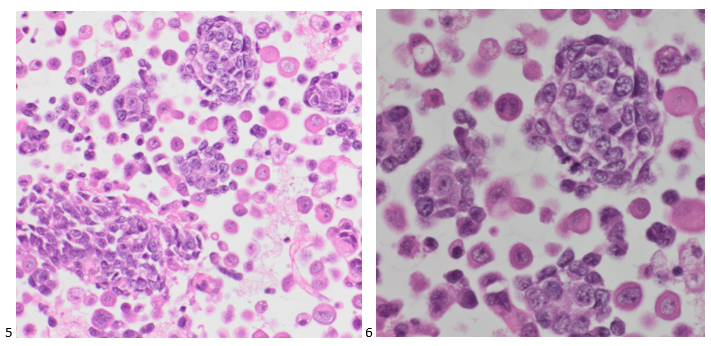
Similar to the Diff-Quik preparation, the small, round cells of interest are forming tight clusters with each cell approximately twice the size of a normal lymphocyte (Image 3). The nuclei are fairly uniform with fine chromatin, relatively small, inconspicuous nucleoli, and scant cytoplasm (Image 2 & 3). The clustering, while not characteristic of this type of tumor, is most likely artifact due to reactivity of being suspended in fluid. What is not pictured in this specimen is the classic Homer-Wright pseudorosettes.
The cell block sections are consistent with the previous cytopreparations, demonstrating a two-cell population. Small, round blue cells (some forming distorted rosettes) in a background of benign-appearing mesothelial cells.
This pleural fluid was diagnosed as positive for malignant cells: consistent with the patient’s known Ewing sarcoma. While immunostains were not necessary for this stage IV diagnosis, the cell block sections are expected to stain positive for CD99 (membranous), vimentin, and FLI1 (as an EWSR1 [22q12] break apart rearrangement (83%) was detected in this patient). A few days after this fluid was signed out, the patient passed away, and his family is now undergoing genetic testing.
-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.