Preface: I wish we lived in a world where cancer did not exist. While I do not foresee that being a reality in my lifetime, I hope I can witness a milestone in oncology when the development of safe and effective therapies surpasses the rate of metastasis. I hope to see the day when instead of being five steps behind cancer, we gain our footing and come out at least one step ahead. We can’t be that far away, right? When I see a patient who is younger than me or around my age, I can’t help but ask myself, “why they have to go through this? Why do they have to be diagnosed with cancer?” Now, they have to choose whether or not to undergo fertility sparing treatment in addition to making a shared decision regarding cytotoxic therapy and radiation. They’re just beginning their life, their career, their family; they’re finally building their story, and it’s interrupted by cancer. Rather than a partner or friend, I see many younger patients present to our clinic with a parent. Imagine how that feels to be a parent – knowing your child was just diagnosed with a terminal disease. How does one cope with that? No parent should have to endure the pain and emotional suffering of losing their child to cancer, let alone anything. We’re meant to outlive our parents, we’re meant to enjoy a full and healthy life, and this case tore right through me.
The patient, a 28 year old male, first presented to an out-of-state health system after managing intermittent right hip discomfort with NSAIDs and ice for three years. When the pain worsened, he went to an urgent care toward the end of 2018, but his X-rays were negative. After his pain became unbearable six months later, he had an MRI which demonstrated a proximal femur lesion with hip and sacral involvement. The femoral lesion biopsied via FNA, and the patient underwent 6 cycles of induction chemotherapy prior to resection. The patient’s PET scan showed improvement, and the 10.5 cm hip mass was resected demonstrating fibrosis and no residual disease. Additional chemotherapy was prescribed for consolidation followed by radiation to the sacral lesions. Seven months after no evidence of disease, a surveillance PET scan demonstrated abundant bone lesions in the arms, ribs, and pelvis. A new relapse chemotherapy regimen was prescribed for refractory disease, but within cycle 2, new calvarial lesions were identified. By the beginning of 2021, the patient underwent stem cell harvesting followed by myeloablative/salvage chemotherapy and an autologous stem cell transplant. Soon after he transferred his care to our institution a few months later, the patient underwent a successful stem cell transplant and remained stable for three months post-transplant. The patient began experiencing severe pain which prompted earlier surveillance imaging, and both PET scan and MRI demonstrated extensive disease progression. To improve comfort and confirm etiology, a right thoracentesis was performed, and 1,200 mL’s of bloody fluid was sent to our cytology lab for analysis. The findings are presented below.
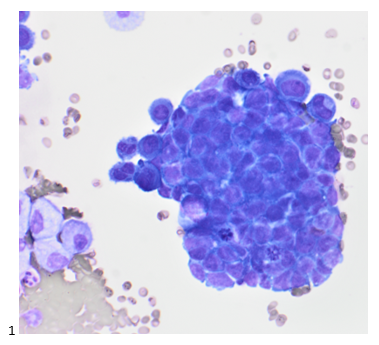
At our institution, we use one or two drops of fresh fluid to make a cytospin for triage purposes. We examine the air-dried, Diff-Quik-stained cytospin to determine whether or not the cells are likely to contaminate our routine preparations, and if the cells are overtly malignant, the remaining cytopreparations need to be stained in our known-positive fluid set-up. In this case, the specimen was deemed routine despite the few clusters of cells that do not resemble the predominating mesothelial cells. The tightly clustered group in Image 1 has small, round nuclei; fine chromatin; scant, blue cytoplasm; and atypical mitoses.
The pap-stained smears and liquid-based SurePath preparation were then screened and the cells of interest highlighted below.

Similar to the Diff-Quik preparation, the small, round cells of interest are forming tight clusters with each cell approximately twice the size of a normal lymphocyte (Image 3). The nuclei are fairly uniform with fine chromatin, relatively small, inconspicuous nucleoli, and scant cytoplasm (Image 2 & 3). The clustering, while not characteristic of this type of tumor, is most likely artifact due to reactivity of being suspended in fluid. What is not pictured in this specimen is the classic Homer-Wright pseudorosettes.
The cell block sections are consistent with the previous cytopreparations, demonstrating a two-cell population. Small, round blue cells (some forming distorted rosettes) in a background of benign-appearing mesothelial cells.
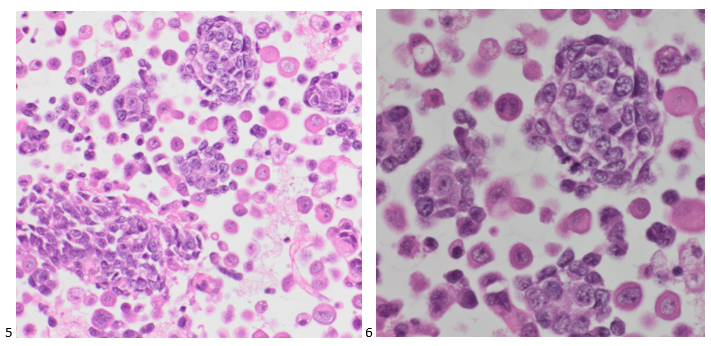
This pleural fluid was diagnosed as positive for malignant cells: consistent with the patient’s known Ewing sarcoma. While immunostains were not necessary for this stage IV diagnosis, the cell block sections are expected to stain positive for CD99 (membranous), vimentin, and FLI1 (as an EWSR1 [22q12] break apart rearrangement (83%) was detected in this patient). A few days after this fluid was signed out, the patient passed away, and his family is now undergoing genetic testing.

-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
