Blue-green cytoplasmic inclusions in neutrophils and monocytes are a novelty in hematology. It is rare to see these inclusions on peripheral smears, and when we do, there is excitement, but sadness too, because, when noted, they usually indicate a poor prognosis and impending death. Thus, we have heard them called “green crystals of death” or “death crystals.” I know I would not want to read a family member’s medical chart and see reference to “death crystals.” It’s an insensitive term, and one the medical community is trying to discourage. And, in fact, though it typically does indicate a poor prognosis, not all cases lead to death. In published reports, it has been shown that short term mortality in patients with these crystals is about 60%.1
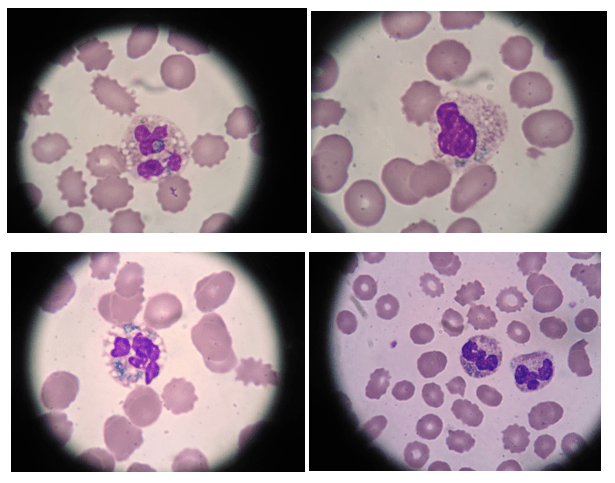
These rare inclusions are refractile and irregular in shape, and are found in neutrophils, and occasionally in monocytes. Color seems to be subjective here. They call them green when inclusions in photos or cells I am looking at look very blue to me. The color perceived may depend on the type of stain (Giemsa, Wright or Wright-Giemsa) used and how fancy we get in color names and descriptions. Or, maybe I’m just color blind! Some people (like my husband) are “lumpers” and call anything blue-green, blue, or green, but don’t recognize subtleties of colors. Thus, I guess to make everyone happy, or to compromise, the blue-green description may fit them best.
These blue-green inclusions were originally reported in patients with hepatic injury and failure. Laboratory results include elevations in AST, ALT and LDH. More recently, there have been cases with no evidence of hepatic injury. Researchers are now finding that these crystals can occur in patients with tissue injury other than liver, and in patients with multiorgan failure. In patients with no liver injury, what is a common factor is that LDH is elevated, indicating tissue injury. Additionally, along with these crystals, lactic acid levels can be used as a predictor of survival. Higher levels of lactic acidosis at the time crystals are noted is a negative predictor of survival.2
In trying to determine the clinical significance of these crystals, they have been subject to a number of different stains to determine their content. The association with hepatic failure led researchers to hypothesize that the crystals were a bile product in circulation. Since then, the crystals have been found to be negative in bile stains. When stained with other stains, Oil Red O showed positive in neutrophils, indicating high lipid content. The inclusions did not stain positive with iron stain or myeloperoxidase. Acid fast stains showed the inclusions to be acid fast positive.3 These crystals also show an interesting similarity to sea-blue histiocytes, which further associates them with tissue injury. After analysis, it is now thought that these crystals contain lipofuscin-like deposits representing lysosomal degradation products, and may be present in multiple types of tissue injury.2
With the current pandemic, I have seen reports of these crystals in COVID-19 patients. I have heard of fellow technologists seeing these, and a recent paper described the first reported cases in patients with COVID-19. These recent incidences may lead to new information about exactly what clinical significance they hold. About one third of COVID-19 patients have elevated ALT and AST, though it is not yet clear whether the liver dysfunction is directly caused by the virus, due to sepsis, or other complications of patient comorbidities. Many COVID-19 patients have mild disease, yet some develop severe pneumonia, respiratory complications, and multiorgan failure. Mortality is increased in these severely affected patients. To better understand and manage treatment for COVID-19, physicians seek to identify biological indicators associated with adverse outcomes.1
In a New York City study, Cantu and colleagues reported on six COVID-19 patients who presented with blue-green crystals in neutrophils and/or monocytes. All six patients had an initial lymphocytopenia, and significantly elevated AST, ALT, LDH and lactic acid at the time the crystals were noted. All of the patients had comorbidities, yet only two of the six presented with acute liver disease. Interestingly, in the six cases reported on in the study, only one had blue-green inclusions reported from the original manual differential. The others were found retrospectively when correlating the cases with patients known to have elevated ALT and AST. All patients died within 20 days of initial diagnosis.1
The consensus of several papers in the last few years is that these crystals are being underreported. As seen in the above study, the crystals were originally seen in just one of the six patients. A look back revealed the other cases. With an increase in COVID-19 cases in our facilities, these blue-green crystal inclusions may be a novelty that is wearing off. We may see a rise in their presence, and need to be able to recognize and report them. This information is important to report if clinicians are to use these crystal inclusions along with acute transaminase and lactic acid elevations to predict poor patient outcomes.
Clinicians, hematologists, and laboratory technologists should be educated and have a high level of awareness of these inclusions. The University of Rochester conducted a study a few years ago that noted that, because these crystals are rare, techs may not be on the lookout for them. Once techs see them, they seem to be on the alert and more are reported. The hospital instituted an “increased awareness” campaign, which resulted in an increase in detection. This revealed cases that were not related to liver injury, including patients with metastatic cancer and sepsis. However, an important correlating factor was that all of the patients had mild to severe elevations in liver enzymes. With more awareness, we are starting to see them in patients without hepatic injury, but with other inflammation and tissue injury.4
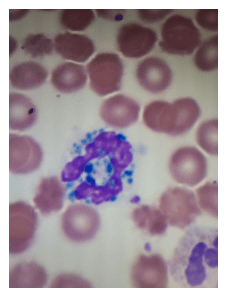
Let’s raise our level of awareness of these maybe-not-so-rare crystal inclusions. And, please be sure to call them by their preferred name, blue-green neutrophil inclusions! Let’s not talk about death crystals or crystals of death.
Many thanks to my colleague Alana D. Swanson, MLS(ASCP)CM , University of Maryland Medical Center and Karen Cable, Hematology Section Lead, Yavapai Regional Medical Center, Arizona, for the photos used in this blog.
References
- Cantu, M, Towne, W, Emmons, F et al. Clinical Significance of blue-green neutrophil and monocyte cytoplasmic inclusions in SARS-CoV-2 positive critically ill patients. Br J Haematol. May 26, 2020.
- Hodgkins, SR, Jones, J. A Case of Blue-Green neutrophil inclusions. ASCLS Today. 2019;32:431.
- Hodgson, T.O., Ruskova, A., Shugg, C.J., McCallum, V.J. and Morison, I.M. Green neutrophil and monocyte inclusions – time to acknowledge and report. Br J Haematol, 2015;170: 229-235.
- Patel,N, Hoffman,CM, Goldman,BJ et al. Green Inclusions in Neutrophils and Monocytes are an Indicator of Acute Liver Injury and High Mortality. Acta Haematol. 2017;138:85-90

-Becky Socha, MS, MLS(ASCP)CM BB CM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 30 years. She’s worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.

Interesting observation. As a cytologist, I have also seen these cases in acute infection and in FNA biopsy. Usually when I have mentioned these inclusions, no one has provided a physiological explanation for their presence. It would be interesting to get a grad student to develop a thesis for their predictive value. Lastly, I think your observation is important because the neutrophil and macrophage cytoplasm, I think, under the proper clinical data, can be used almost like an immuno-histochemisty test to determine what the immune system is encountering. The correlation between Covid 19 patients with elevated ALT and AST, along with the other associated background cells (i.e. monocytes) and cytoplasmic inclusions of the macrophage and neutrophils could be used as a diagnostic biomarker or to determine therapeutic approach and risk factor. In fact, I may write to UCSD or CSU to see if this could be considered for investigation.
That does sound like a great research project! I’d love to see that. Thanks for your comments!