Case History
A sixty nine year old female who underwent right breast reconstruction about 13 years ago due to breast cancer presents to the doctor office with right breast pain and right breast enlargement over the last two months. She has lost some weight and does not recall any trauma to this area. She had a textured saline implant. Examination reveals no definite palpable masses. MRI of right breast showed intact saline implant with moderate amount of fluid surrounding the implant within the intact external capsule. No adenopathy was noted. Right breast implant was removed and complete capsulectomy was performed.
Diagnosis
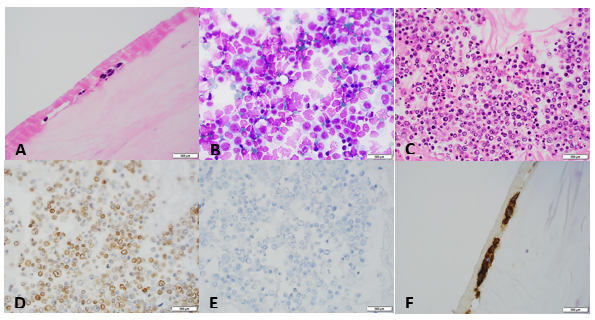
Breast implant-associated anaplastic large cell lymphoma.
Discussion
Breast implant associated anaplastic large cell lymphoma is a provisional entity that is morphologically and immunophenotypically similar to ALK-negative anaplastic large cell lymphoma. It arises primarily in association with a breast implant. It is a very rare entity with an incidence of 1 in 500,000 to 3 million women with implants. Tumor cells may be localized to the seroma cavity or may involve pericapsular fibrous tissue. Sometimes it can form a mass lesion. Locoregional lymph node may be involved. The mean patient age is 50 years. Most patient presents with stage 1 disease, usually with peri-implant effusion. The mean interval from implant placement to lymphoma diagnosis is 10.9 years. There is no association with the type of implant. Histologic examination shows two different types of proliferations. In patients with seroma, the proliferation is confined to the fibrous capsule (“in situ” iALCL). However, the distribution of neoplastic lymphocytes could be heterogeneous with some cellular areas with numerous large pleomorphic cells of varying size and some fibrotic areas with rare atypical lymphocytes. It is beneficial to look at the seroma fluid in addition to capsule sections, because sometimes the neoplastic lymphocytes are predominantly present in fluid (as in our case). Patients presenting with tumor mass show more heterogeneous proliferations infiltrating surrounding tissues (“infiltrative” iALCL). They consists of either sheets are clusters of large neoplastic cells accompanied by a large number of eosinophils. By immunohistochemistry, the tumor cells are strongly positive for CD30. CD2 and CD3 are more often positive than CD5. CD43 is almost always expressed. Most cases are CD4 positive. The prognosis is very good in patients with disease confined to the capsule. The median overall survival is 12 years. However, patients with a tumor mass could have a more aggressive clinical outcome.
References
1. Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues (Revised 4th edition). IARC: Lyon 2017.
2. Jaffe, E , Arber, D, et al. Hematopathology (second edition) 2017.

-Junaid Baqai, MD, was born in Chicago, IL but spent most of his life in Karachi, Pakistan. He graduated from DOW Medical College in Pakistan and did his residency in anatomic and clinical pathology at Danbury Hospital, CT followed by hematopathology fellowship from William Beaumont Hospital, Michigan and oncologic-surgical pathology fellowship from Roswell Park Cancer Institute, New York. He currently serves as Medical Director of hematology, coagulation and flow cytometry at Memorial Medical Center and Medical Director of Laboratory at Taylorville Memorial Hospital.

I have worked for a long time with a murine model…NPM-ALK.Any clue regarding the molecular basis of this tumor?