Case History
An 85 year old man presented with pancytopenia and weakness. His labs include WBC of 3.2, HgB of 9.9 and platelets of 137.
Bone Marrow Biopsy



Flow Cytometry


Diagnosis
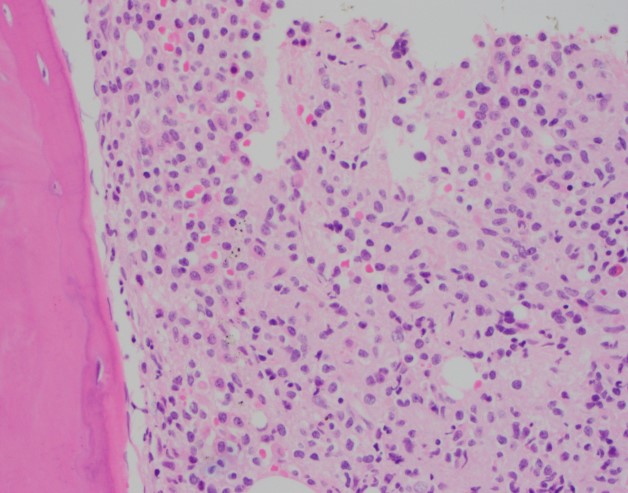
The bone marrow aspirate shows multiple cellular spicules with a prominent population of lymphoid cells with oval to reniform nuclei, dispersed chromatin and abundant pale cytoplasm. Scattered plasma cells are also present.
The core biopsy shows an infiltrating population of atypical lymphocytes with moderate amounts of pale eosinophilic cytoplasm and mature chromatin that stain positive for CD20. Frequent mononuclear cells consistent with plasma cells are also seen scattered throughout the bone marrow and stain positive for CD138.
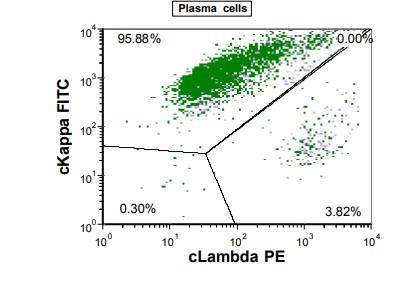
Flow cytometry revealed that 80% of the lymphoid gate represented a kappa light chain restricted population that co-expressed B-cell markers CD19, CD20 and CD22 along with classic hairy cell leukemia specific markers CD11c, CD25 and CD103. A second population of kappa restricted cells fell in the plasma cell gate. The cells co-expressed CD138, CD56 and were largely negative for CD19 and CD20.
Overall, there is a hypercellular bone marrow with a prominent mononuclear lymphoid infiltrate consistent with hairy cell leukemia and a concurrent population of plasma cells consistent with plasma cell neoplasm.
Discussion
Hairy cell leukemia is a rare lymphoid neoplasm that accounts for only 2% of lymphoid leukemias. Patients tend to be in their 50s-60s with a 4:1 male predominance. The tumor is generally found in the bone marrow and spleen with rare circulating cells in the peripheral blood. Patients are generally cytopenic at presentation and symptoms include weakness and fatigue. Splenomegaly is common and hepatomegaly can also be seen.. 1
Hairy cell leukemia involves the clonal expansion of B-cells with a unique immunophenotypic profile. They are bright for CD19, CD20, CD22 and CD200, negative or dim for CD5, CD23 and CD10 and positive for CD11c, CD103, CD123 and CD25. Hairy cell leukemia must be distinguished from two provisional entities, hairy cell leukemia-variant and splenic diffuse red pulp lymphoma. These two entities do not have the classic morphology or staining profile of hairy cell leukemia.2
BRAF V600E mutations are detected in more than 80% of cases of classic hairy cell leukemia. The mutation is considered to be a driver mutation, but additional mutations are usually present that lead to disease progression. Hairy cell leukemia-variant is usually negative for BRAF mutations and has a more aggressive clinical course.3
Patients with hairy cell leukemia are given purine analogues as first line treatment and generally do well. However, patients who do not respond or who undergo relapse have few options. Increasingly, BRAF V600E inhibitors are being used for patients with hairy cell leukemia. Multiple studies have now confirmed the efficacy of vemurafenib and dabrafenib, however patients can be quick to relapse once off the drugs. Combination approaches should be considered for the most effective treatment. 4
References
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues (Revised 4th edition). IARC: Lyon 2017.
- Troussard X, Cornet E. Hairy cell leukemia 2018: Update on diagnosis, risk‐stratification, and treatment. American Journal of Hematology. 2017;92(12):1382-1390. doi:10.1002/ajh.24936.
- Maitre E, Bertrand P, Maingonnat C, et al. New generation sequencing of targeted genes in the classical and the variant form of hairy cell leukemia highlights mutations in epigenetic regulation genes. Oncotarget. 2018;9(48):28866-28876. doi:10.18632/oncotarget.25601.
- Roider T, Falini B, Dietrich S. Recent advances in understanding and managing hairy cell leukemia. F1000Research. 2018;7:F1000 Faculty Rev-509. doi:10.12688/f1000research.13265.1.

–Chelsea Marcus, MD is a third year resident in anatomic and clinical pathology at Beth Israel Deaconess Medical Center in Boston, MA and will be starting her fellowship in Hematopathology at BIDMC in July. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
