Hello again readers. It’s been a while as I took some time off from blogging. But I hope to update you every once in a while when I can. So, I’m currently in my final year of residency and have been serving as chief since April 1st. My chief term ends before the end of the year to provide time to focus on studying for the boards (we take our boards in mid-May).
When I reminisce about residency, I can’t believe that almost four years have flown by so quickly. I remember arriving in Chicago for a 2 week boot camp we had prior to our start date on July 1st just like it was yesterday. It was nice to be back in a familiar city (The University of Chicago is my alma mater), although many things had changed in the two decades since I had last been a college student in the Windy City.
Thinking about it now, I really appreciate all the thought and hard work that my director of surgical pathology, Dr. Elizabeth Wiley, had put into organizing this boot camp to ease us into the transition to residency (and surgical pathology). We learned Rokitansky method of autopsy dissection on 3 pig blocks that she personally picked up from the butcher’s for us and later had to complete a competency exam by ourselves on a 4th pig block. We learned to cut frozen sections on various tissues from our pig blocks (and of course, had a competency exam on that as well). We learned to gross uteri and prostates on ground turkey versions (complete with chickpea leiomyomas) that she and her fellows had made for us. We had weekly online exams on histology (we had a slide scanner which I now appreciate that not everyone has one) and special didactics on surgical pathology topics we don’t see much during general sign-out (dermatopathology, neuropathology, hepatopathology, and nephropathology) in addition to the usual goings-on during a surgical pathology rotation. We eventually had online modules on surgical pathology as well. And of course, we had three months straight (I hear its five months now) of learning to gross with our awesome fellows. I now appreciate more deeply just how innovative and dedicated Dr. Wiley was to our surgical pathology education. And even though I ultimately chose to pursue fellowships in hematopathology and molecular genetic pathology, the foundation in surgical pathology that was established during that boot camp still helps and influences me now.
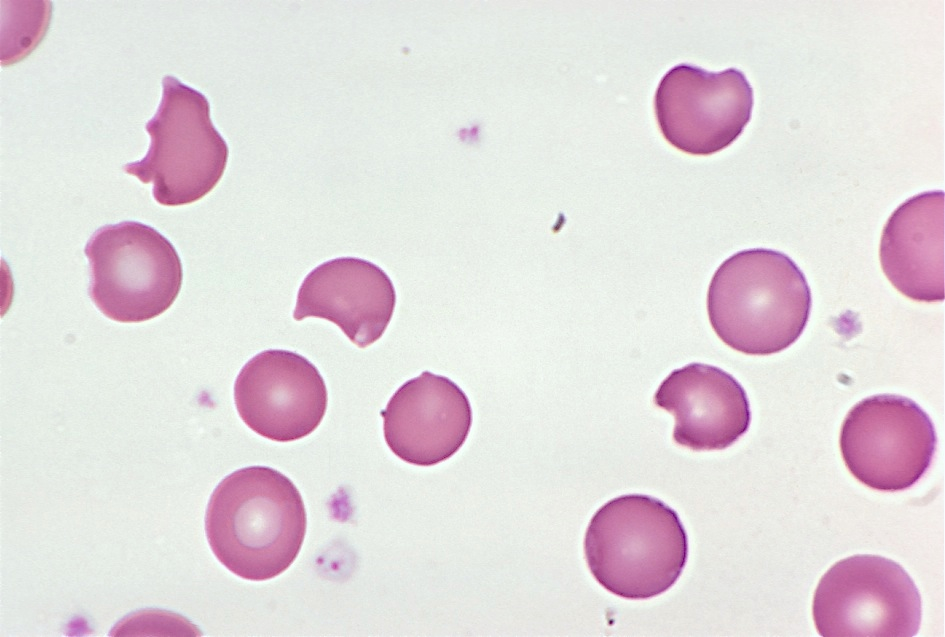
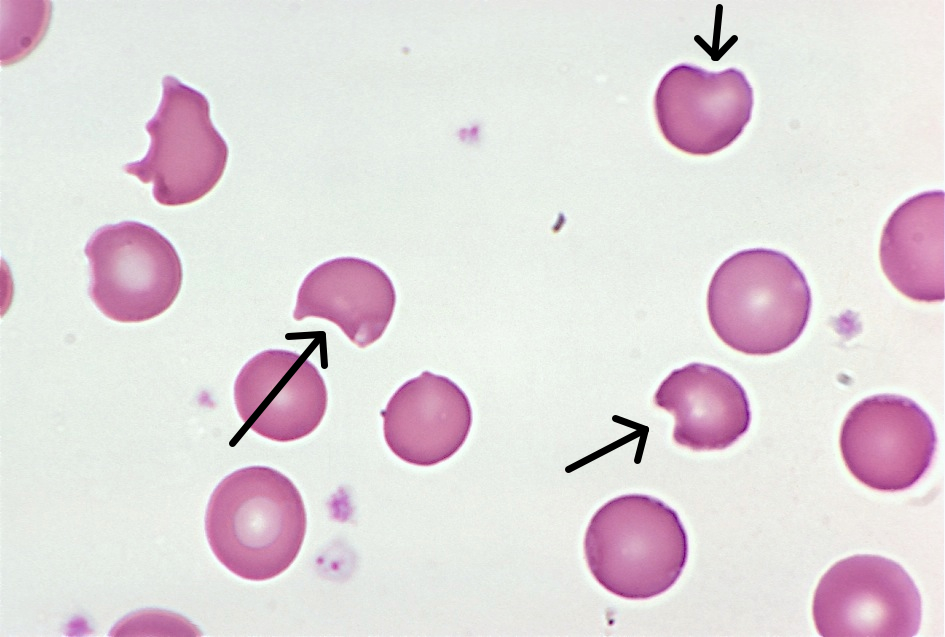
During my first year, I was also fortunate to have hematopathology at Jesse Brown VA Medical Center with Dr. John Kennedy. He is a hematopathologist who was trained as a morphologist before the heavy reliance on flow cytometry and IHC. And he taught me to love the morphology of blood cells especially with respect to lymphomas. I had enjoyed my hematology sub-I at the NIH when I was a medical student but had originally entered residency thinking that I’d pursue molecular genetic pathology and clinical microbiology. But a great mentor can really open your mind to a different path and that is what Dr. Kennedy did for me. The second time I rotated with him, he was away for much of the rotation. But I loved the opportunity that I was given to take care of the hematopathology service in his absence. I looked at all the daily cases and performed path reviews and counts on peripheral blood smears and body fluids and the surgical pathology attending at the end of the day would review and sign-out my work. This experience of graduated responsibility helped me to decide to pursue hematopathology and it was nice to have someone believe in me and my abilities. I was also fortunate that I was in a city where the Lymphoma Foundation also held quarterly inter-program Lymphoma Rounds which I was able to attend.
So my advice is to identify mentors early on in your residency. You may not be able to see the ripple effect they have on your life until later on but I promise that they will touch your lives in an indelible manner that will help shape the pathologist you will become later on in life.
This week I’m at the ASCP Annual Meeting and will write about those experiences in a future blog, but for now, I’d like to take this opportunity to personally thank my mentors. I hope that I take your lessons and make you proud as a future physician-scientist with a public health (molecular epidemiology aka biomarker discovery which was one of my areas of specialization during my MPH) focus. You have touched my life in ways that I may not always be able to articulate but do acknowledge and appreciate.

-Betty Chung, DO, MPH, MA is a fourth year resident physician at Rutgers – Robert Wood Johnson University Hospital in New Brunswick, NJ.