A 59-year-old man presented to the Emergency Room with bright red blood per rectum, associated with nausea, vomiting, abdominal cramping, and persistent watery diarrhea. Several days earlier, he had returned from a three-week trip to the Dominican Republic. On physical examination, he was afebrile. His abdomen was soft and not tender or distended.
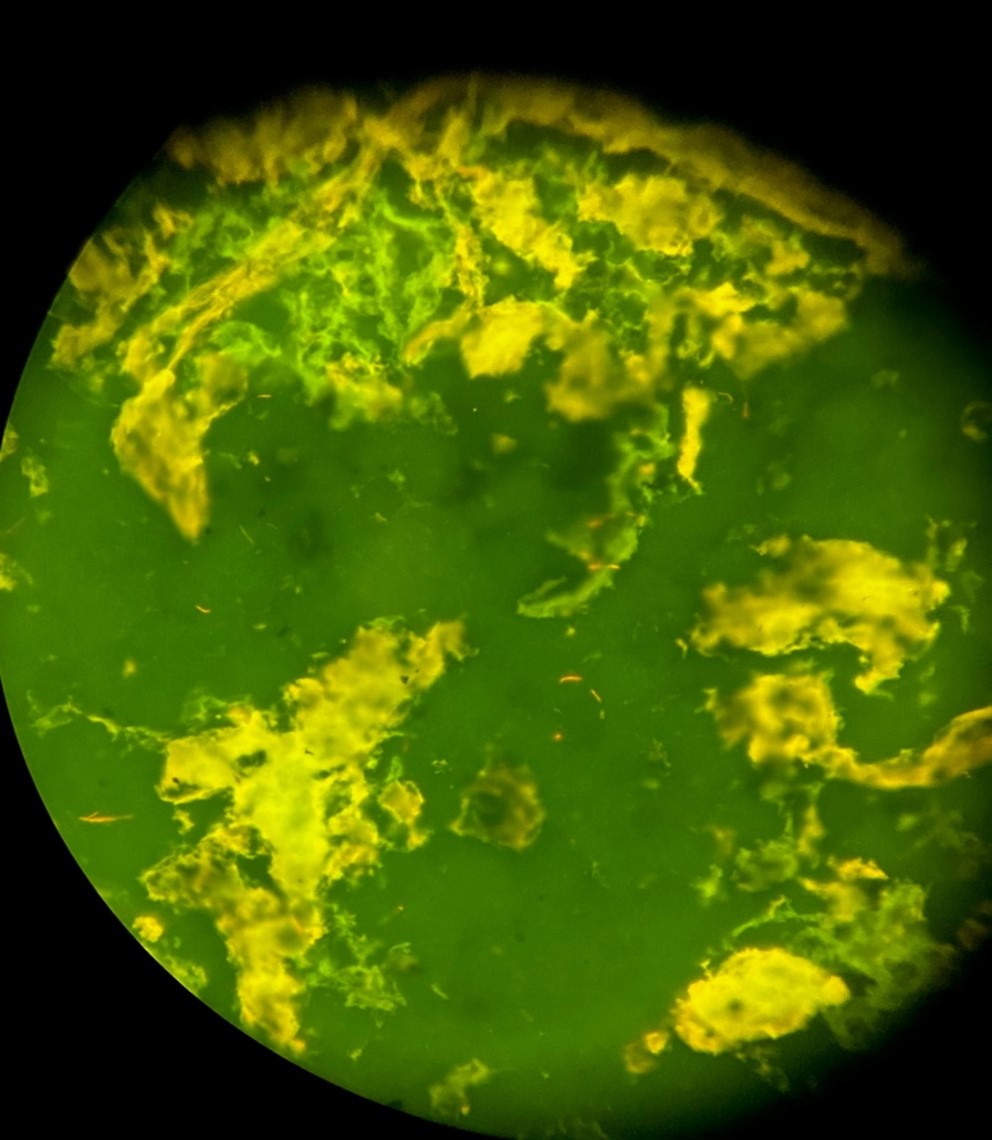
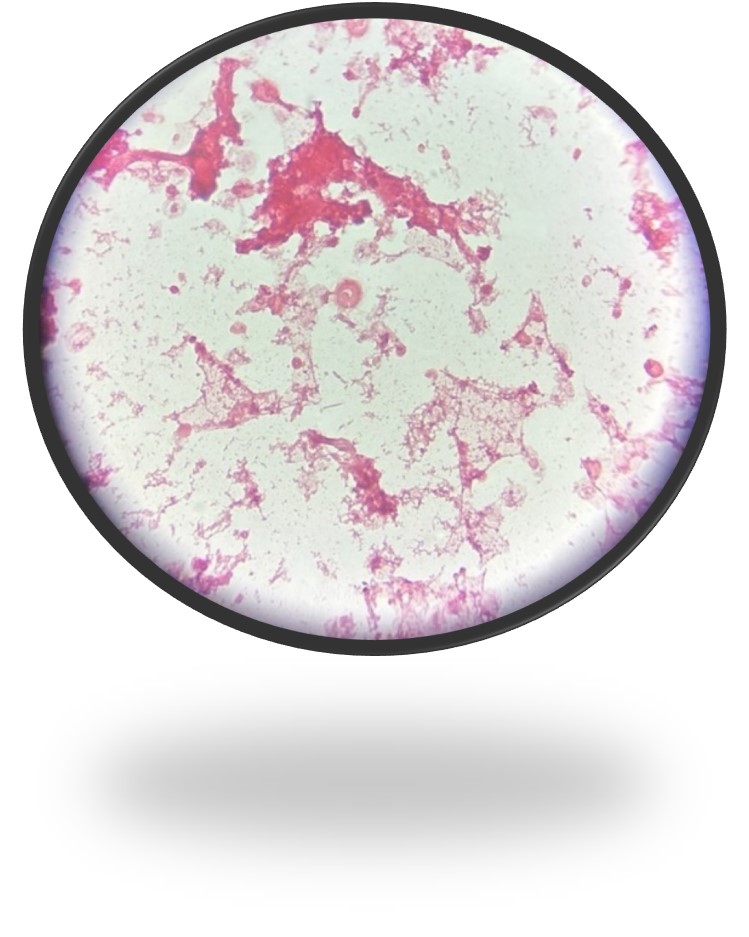
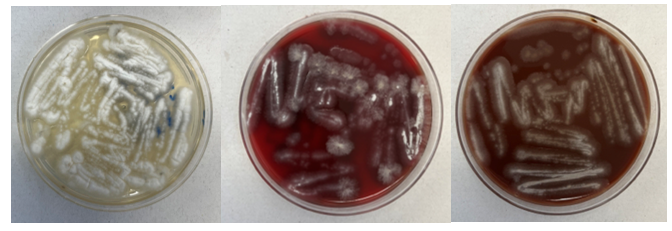
A stool sample was sent to the Microbiology Lab for PCR testing, and both Vibrio and Vibrio cholera targets were detected. The stool was then plated for culture confirmation. Hemolytic colonies grew on the blood agar plate (Figure 1), and yellow (original medium color green) colonies grew on thiosulfate citrate bile sucrose selective agar due to sucrose fermentation (Figure 2). Gram stain from these colonies showed gram negative, curved, comma-shaped rods (Figure 3) and MALDI-ToF identification revealed Vibrio albensis. The specimen was sent to the Department of Public Health for confirmation, which reported Vibrio cholerae O1 serovar Ogawa with O1 antigen typing.
Vibrio albensis is a gram negative, halophilic bacterium belonging to the Vibrionaceae family. V. albensis is a recently identified species within the Vibrio genus and is believed to be a member of the Vibrio cholera complex. Although primarily considered non-pathogenic, V. albensis has been associated with rare cases of human infections, particularly in individuals with compromised immune systems.1 While previously reported studies indicated V. albensis as a non-O1, non-O130 serogroup of V. cholerae,2the Department of Public Health confirmed our patient’s isolate as O1 serovar Ogawa by O1 antigen typing. V. albensis is an emerging pathogen with limited information regarding its clinical significance and optimal management. The infections are predominantly associated with contaminated seawater or seafood exposure. The primary transmission mode is through open wounds or ingesting raw or undercooked seafood.3
Clinical presentation of this organism can be similar to V. cholerae, as diffuse watery diarrhea, the hallmark of cholera, or asymptomatic. Other case reports presented bacteremia, septicemia, and urinary tract infections.4,5
Laboratory diagnosis of Vibrio cholerae albensis infection involves isolating and identifying the bacterium from stool samples. This can be achieved using selective culture media, such as thiosulfate-citrate-bile salts-sucrose (TCBS) agar, which allows for the growth of V. cholerae and its variants.6
Antimicrobial resistance is a growing concern in the management of cholera. Studies have reported varying resistance levels to commonly used antibiotics in V. cholerae, including V. cholerae albensis. It is essential to monitor antimicrobial susceptibility patterns to guide appropriate treatment strategies.7 Further research is needed to better understand the epidemiology, clinical manifestations, and optimal treatment strategies for V. albensis infections as members of V. cholerae complex are being identified/recognized with more advanced diagnostic tools.
References
Baker-Austin C, et al. (2016). Vibrio albensis sp isolated from a mesophilic bacterial culture, abalone (Haliotis spp.), and seawater. International Journal of Systematic and Evolutionary Microbiology, 66(1), 187-192.
Ahmed AOE, Ali GA, Hassen SS, Goravey W. Vibrio albensis bacteremia: A case report and systematic review. IDCases. 2022 Jun 30;29:e01551. doi: 10.1016/j.idcr.2022.e01551. PMID: 35845827; PMCID: PMC9283503.
3. Sharma P, et al. (2018). Vibrio albensis: An Emerging Pathogen Causing Necrotizing Fasciitis. Journal of Clinical Microbiology, 56(3), e01454-17.
4. Araj GF, Taleb R, El Beayni NK, Goksu E. Vibrio albensis: An unusual urinary tract infection in a healthy male. J Infect Public Health. 2019 Sep-Oct;12(5):712-713. doi: 10.1016/j.jiph.2019.03.018. Epub 2019 Apr 10. PMID: 30981654.
5. Sack RB, et al. (2004). Cholera. The Lancet, 363(9404), 223–233.
6. Centers for Disease Control and Prevention (CDC). (2021). Laboratory Methods for the Diagnosis of Vibrio cholerae. Retrieved from https://www.cdc.gov/cholera/laboratory.html
7. Ceccarelli, M., et al. “Editorial–Differences and similarities between Severe Acute Respiratory Syndrome (SARS)-CoronaVirus (CoV) and SARS-CoV-2. Would a rose by another name smell as sweet.” European review for medical and pharmacological sciences 24.5 (2020): 2781-2783.
-Eros Qama, MD, is a 2nd year AP/CP pathology resident in the Department of Pathology at Montefiore Medical Center in Bronx, NY
-Phyu Thwe, Ph.D, D(ABMM), MLS(ASCP)CM is Associate Director of Infectious Disease Testing Laboratory at Montefiore Medical Center, Bronx, NY. She completed her medical and public health microbiology fellowship in University of Texas Medical Branch (UTMB), Galveston, TX. Her interests includes appropriate test utilization, diagnostic stewardship, development of molecular infectious disease testing, and extrapulmonary tuberculosis.
An 83 year old female with history of type 2 diabetes presented to the emergency room (ER) with two month history of dysuria and diarrhea. Upon admission, Clostridiodes difficile (C. difficile ) GDH/TOX with reflex to nucleic acid amplification test (NAAT), urine culture, and 2 sets of blood culture specimens were collected for testing. C. difficile test was positive for GDH and Toxin A/B production. Urine culture was positive with 50,000 – 99,000 colony forming units (CFU)/mL of Klebsiella pneumoniae. Patient was administered ceftriaxone, metronidazole and vancomycin and discharged three days post admission. On day of discharge, blood cultures were documented as “no growth at 3 days”. The patient visited her primary care physician the day after discharge. Two days later, the primary care office was notified of a corrected report. The patient’s blood culture collected on day of admission was being corrected from no growth to a positive with growth of Fusobacterium nucleatum. The patient was contacted to check on her status and medication compliance was verified. Patient continued to demonstrate symptom improvement during follow up at physician’s office 10 days post discharge.
What happened here?
The blood culture was collected at an acute care hospital. The system microbiology laboratory policy for a first blood culture positive that is read as no organisms seen (NOS) from an acute care hospital laboratory, is to inoculate appropriate media and prepare three smears. Gram stain is to be performed on one of the smears and if organisms are not seen, a stained and unstained smear, along with inoculated media, are to be sent to the core microbiology laboratory (core lab). The bottle is then to be reloaded on the blood culture instrument.
The policy for a second positive alert from the same NOS bottle is to inoculate appropriate media and prepare 3 cytospin smears. Gram stain is to be performed on one of the cyto-smears and if organisms are still not seen, a stained and unstained smear are to be sent to the core lab along with the positive bottle and inoculated media. The core lab is to use the unstained cytospin smear to make and read an acridine orange (AO) stain.
In this patient’s case, the anaerobic blood culture bottle from one set flagged as positive on day 4 of incubation. The gram stain was read as NOS and inoculated media and smears were sent to the core lab. The bottle was reloaded on the instrument and the bottle alerted as positive a second time that day. The cytospin gram stain was read as NOS and inoculated media, smears, and blood culture bottle were sent to the core lab. At the core lab, a new unspun smear was made from the bottle. AO was performed on this smear and read as NOS.
In our laboratory, if a gram stain result is not entered for a blood culture, it will auto verify as a negative blood culture every 24 hours with a final negative result at 5 days. Both blood culture sets on this patient resulted as no growth at 5 days.
At the 48 hour (6 days post-collection) culture read, BAP, CHOC, and MAC demonstrated no growth, but the CDC ANA had growth. The isolate was setup for MALDI identification and resulted as 99.9% Fusobacterium nucleatum.
Per protocol, a review of smears was performed on this discrepant smear-culture. The unstained cyto-smear sent by the acute care laboratory had not been stained with AO and read per protocol. Rather, as was mentioned above a Gram stain was made on a new unspun smear and read as NOS. Reviewing this AO stain during the investigation revealed long thin fluorescing rods with tapered ends (Fig 1)
The cyto-smear that had been sent after the second positive alert, but did not get stained and read was also stained with AO and long thin fluorescing rods with tapered ends were observed (Fig 2).
At this point in the investigation, the unspun gram stain from the 1st positive alert that was sent over from the acute care hospital laboratory was also reviewed. Knowing that the bottle was positive for F. nucleatum the technologist shared that she eventually saw rare long thin gram-negative rods with pointed ends that matched what was seen in the AO (Fig 3). As part of the investigation, safranin was added for an additional 10 minutes revealing the organism more clearly (Fig 4).
Figure 1. Acridine orange of unspun slide. Figure 2. Acridine orange of cytosmearFigure 3. Gram stain of unspun smear. Figure 4. Gram stain of unspun smear with 10 minutes of safranin
Discussion
Fusobacterium is an obligate anaerobic gram-negative rod that gram stains as a light staining thin rod with pointed ends. Fusobacterium are found in oropharyngeal flora and are commonly seen in oral biofilms. It is a primary pathogen seen in peri-implantitis, root canal infections, dentoalveolar abscesses and spreading odontogenic infections. It can also be a pathogen seen in abscesses in various parts of the body and seen in the blood stream.
Due to the staining characteristics of Fusobacterium species, they often blend into the background of gram stains from positive blood cultures. As a result, the miss in gram stain and delay in culture growth combined with the late detection of Fusobacterium on blood culture instrumentation for these fastidious organisms can result in a false negative report that is only caught after the organism grows from the original NOS bottle.
Safranin is a secondary stain or counterstain, utilized in the Gram stain, that will stain the colorless gram negative bacteria pink or red. Legionella, Brucella melitensis, Legionella and Campylobacter species are all reported to be enhanced with safranin left on for 2 minutes and it is recommended if anaerobes are suspected and not seen to leave on for 3-5 minutes or use basic fuchsin in order to enhance the morphology of these organisms. For this reason, some laboratories routinely use basic fuchsin as the counterstain.
Acridine orange (AO) is a fluorochromatic dye which binds to nucleic acids of microorganisms and human cells. Acridine orange is a fluorochrome stain that binds to the nucleic acid of cells and bacteria. RNA and single‐stranded DNA will appear orange and double‐stranded DNA found in human cells, with the exception of red blood cells, will appear yellow or yellow‐green, when visualized under UV light. Therefore, bacteria and fungi stain bright orange while epithelial, white blood cells, and background debris will appear pale green to yellow. To name a few, some common applications for AO include routine screening of normally sterile body fluids and rule‐out of Gram‐positive microorganisms versus crystal violet stain precipitate. Of important note, while not able to differentiate the actual organism, it does work for detecting Mycoplasma and Ureaplasma.
Conclusion
Blind subculturing of NOS gram stains from positive blood cultures, longer staining with safranin, and AO stains are beneficial to be added to the micro lab armamentarium. They are especially beneficial when added into the protocol for processing sterile body site specimens in which organisms, that stain lightly and blend in the background, may be suspected. For further review, Special Media or Stains for Fastidious and Infrequently Encountered Organisms can be found in the Clinical Microbiology Procedures Handbook 5th edition.
References
Kononen E, Nagy E, Conrads G. 2023. Bacteroides, Porphyromonas, Prevotella, Fusobacterium, and Other Anaerobic Gram-Negative Rods. Manual of Clinical Microbiology 13th edition. ASM Press, Washington, DC.
Tille PM. Bailey & Scott Diagnostics Microbiology, 14th ed., St. Louise, Mosby, Inc., 2017.
Dallas SD and Harrington A. 2023. 3.2 Staining Procedures. Clinical Microbiology Procedures Handbook 5th edition. ASM Press, Washington, DC.
-Jennifer Tedrick MLS(ASCP), Technical Specialist
-Maureen Bythrow, M(ASCP), Microbiology Manager
-Frances Valencia-Shelton, PhD, D(ABMM), SM(ASCP)CM is the Clinical Infectious Diagnostics Director for the Baptist Health System in Jacksonville, FL. She is actively engaged in the Jacksonville Area Microbiology Society and the American Society for Microbiology. Her interests include defining and utilizing clinical best-practice for testing and reporting. She is equally interested in learning with and educating others in the field of clinical microbiology.
A 62 year old male, former smoker, with status post double lung transplant three months prior, presented to the lung transplant clinic for a follow-up appointment in July complaining of shortness of breath, which had worsened over the past 3 weeks and prompted the need for O2 again with minimal daily activities. He denies any chest pain, fevers, headaches, dizziness, N/V/D. He was admitted for further management of possible organ rejection and worsening respiratory function tests.
The patient was started on IV solumedrol followed by a prednisone taper. A chest CT (non-contrast) showed patent bronchial anastomoses and stable bilateral small right greater than left loculated pleural effusions. Respiratory pathogen panel results were negative, and Cryptococcus Antigen and titer were negative. He then underwent bronchoscopy and biopsy, showing no signs of rejection. BAL was sent to microbiology for cultures. Fungal culture grew 3 days after incubation (Fig 1), and the Lactophenol cotton blue (LCB) prep shows septate hyphae with long and short conidiophores in small groups, which was identified as Scedosporium spp.
Figure 1: (left to right) Sabouraud agar, Blood agar, Chocolate AgarFigure 2: Lactophenol cotton blue (left) low magnification and (right) high magnification
Discussion
Scedosporium apiospermum is an environmental mold increasingly reported as an opportunist organism due to the increasing use of corticosteroids, immunosuppressants, antineoplastics, and indiscriminate use of broad-spectrum antibiotics.1 The organism can cause various diseases, including colonization in cystic fibrosis, neurological infection associated with near-drowning incidents, and disseminated disease in immunocompromised individuals.2,3
Laboratory diagnosis of a Scedosporium infection is primarily based on the histopathologic exam from a direct specimen or microscopic examination of lactophenol cotton blue prep of fungal culture growth combined with the clinical or radiographic findings suggesting infection. Since the microconidia of Scedosporium could resemble Blastomyces spp, care should be taken to rule out the dimorphic mold. Scedosporium grows well and faster than Blastomyces on routine mycological media such as Sabouraud’s glucose agar, blood agar, and chocolate agar. Patient’s travel/demographic history is particularly important since Blastomyces is commonly found in Ohio and Mississippi River Valley regions and endemic in Southcentral and Southeastern US whereas Scedosporium is ubiquitous.4
Scedosporium growth is also observed on the media with a high concentration of cycloheximide5 which is inhibitory for clinical Aspergillus species. A competing fungal flora of rapidly growing Aspergillus and Candida species is frequently present. Isolation using benomyl agar6 or cycloheximide-containing agar is then recommended. Culture of sputum or bronchoalveolar lavage (BAL) or secretions from the trachea or external ears, particularly in CF patients, may be hampered by their mucoid consistency.
Typically, fungal identification is achieved primarily via microscopic examination in clinical microbiology laboratories. At the same time, more laboratories have adopted matrix-assisted laser-desorption-ionization Time-of-Flight (MALDI-ToF) for more accurate and rapid identification. Microscopic examination from a fungal culture requires a significantly longer time for mold sporulation. With MALDI-ToF, identification can be achieved rapidly as soon as sufficient growth for protein extraction. Nucleic-acid-based identification methods, such as DNA polymerase chain reaction (PCR) combined with ITS (Internal transcribed spacer) or 28s rRNA, can also be used for identification directly from clinical samples or the mold grown on culture.7 Histopathologic examination is helpful for determining the presence of invasive mold infection, but it is not possible to establish definitive identification without culture because various hyaline molds have a similar appearance. For this reason, culture is still an essential part of the diagnostic evaluation. Culture is also vital for testing in vitro susceptibility since Scedosporium spp can be resistant to multiple antifungal agents.7
References
[1] Khan A, El-Charabaty E, El-Sayegh S. Fungal infections in renal transplant patients. J Clin Med Res. 2015;7:371–8.
[2] K.J. Cortez, E. Roilides, F. Quiroz-Telles, J. Meletiadis, C. Antachopoulos, T. Knudsen, et al. Infections caused by Scedosporium spp Clin Microbiol Rev, 21 (1) (2008), pp. 157-197
[3] W.J. Steinbach, J.R. Perfect Scedosporium species infections and treatments J Chemother, 15 (2003), pp. 16-27
[4] Kim MK, Smedberg JR, Boyce RM, Miller MB. The Brief Case: “Great Pretender”-Disseminated Blastomycosis in Western North Carolina. J Clin Microbiol. 2021 Nov 18;59(12):e0304920. doi: 10.1128/JCM.03049-20. Epub 2021 Nov 18. PMID: 34792387; PMCID: PMC8601235.
[5] Rippon JW. , Medical Mycology. The Pathogenic Fungi and the Pathogenic Actinomycetes3rd edn, 1998PhiladelphiaSaunders
[6] Summerbell RC. The benomyl test as a fundamental diagnostic method for medical mycology, J Clin Microbiol, 1993, vol. 31 (pg. 572-577)
[7] De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, Pappas, et al. European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group; National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008 Jun 15;46(12):1813-21. doi: 10.1086/588660. PMID: 18462102; PMCID: PMC2671227.
-Abdon Lopez Torres, M.D., is a second year AP/CP resident of Pathology Department at Montefiore Medical Center, Bronx, NY. He completed his medical degree in Saint George’s University in Grenada. He’s interested in pursuing a surgical pathology fellowship after completing his residency.
-Phyu Thwe, Ph.D, D(ABMM), MLS(ASCP)CM is Associate Director of Infectious Disease Testing Laboratory at Montefiore Medical Center, Bronx, NY. She completed her medical and public health microbiology fellowship in University of Texas Medical Branch (UTMB), Galveston, TX. Her interests includes appropriate test utilization, diagnostic stewardship, development of molecular infectious disease testing, and extrapulmonary tuberculosis.
A 35 year old female patient with a past medical history of uncontrolled HIV, retinitis caused by cytomegalovirus and recurrent colitis presented to the Emergency Department with body pain, fever, severe neutropenia, and diarrhea. CT scan revealed worsening sigmoid/rectal wall thickening. Patient also presented with esophageal candidiasis. Blood workup revealed that the patient had sickle cell disease (HBSC), anemia (Hgb 5.6 gm/dl) that required multiple transfusions, and elevated white blood cell count (up to 17,000). The patient also had leukopenia (neutropenia and lymphopenia), which, in addition to the anemia without hemolysis or bone marrow compensation and CD4 count <50, led to strong suspicious of disseminated mycobacteria infection. A bone marrow biopsy was performed and AFB staining revealed loose granulomas and numerous acid-fast bacilli seen. Culture of the bone marrow grew out acid-fast bacilli further identified as Mycobacterium avium complex (MAC).
Discussion
Mycobacterium avium complex (MAC) is made up of several nontuberculosis mycobacterial (NTM) species that require genetic testing to be speciated.1 MAC is predominantly made of the slow-growers mycobacteria (SGM) such as M. avium, M. intracellulare, M. chimaera, and M. colombiense.2,3 Most species of nontuberculosis mycobacteria are found in environmental sources. The MAC organisms are found throughout the environment, particularly in the soil and water, mainly in the Southeast of the United States.1Human diseases are most likely from exposure to environmental sources either through direct inhalation, implantation or indirect consumption or contamination food or water. MAC is considered the most commonly encountered group of slow growers.
The MAC cause pulmonary disease that is clinically similar to tuberculosis, mostly in immunocompromised patients with CD4 cell counts less than 200/μL, such as those with HIV/AIDS. They are the most frequent bacterial cause of illness in patients with HIV/AIDS and immunosuppression.1,4 MAC is also the most common nontuberculosis mycobacterial species responsible for cervical lymphadenitis in children. Additionally, hypersensitivity pneumonitis-like symptoms can occur which were initially thought to be an allergic reaction only, but current studies suggests infection and inflammation. Traditionally, MAC cause chronic respiratory disease, populations such as middle-aged male smokers and postmenopausal females with bronchiectasis (also known as Lady Windermere syndrome).
Diagnostic testing for pulmonary infection caused by MAC includes acid-fast bacillus (AFB) staining and culturing of the appropriate specimens. Respiratory specimens are the most commonly tested specimen type. If disseminated MAC (DMAC) infection is suspected, culture specimens should include blood and urine. Blood cultures are typically used to confirm the diagnosis of DMAC in an immunocompromised patient with clinical signs and symptoms 5. MAC can also be isolated from bodily fluids and other tissues, such as lymph nodes and bone marrow. If diarrhea is present, stool cultures can be collected. Skin lesions should be cultured if clinically warranted. To determine pulmonary involvement, imaging studies of the chest should be performed. Lymph node biopsy or complete lymph node excision is usually used to diagnose MAC lymphadenitis in children. Skin testing (MAC tuberculin test) has little value in establishing a diagnosis.6 Routine screening for MAC in respiratory or GI specimens is not recommended.
Organisms part of the MAC are not stained well by the dyes used in Gram stain, but instead are acid-fast positive. The ability of an organism to hold onto the carbol-fuchsin stain after being treated with a mixture of ethanol and hydrochloric acid is referred to as “acid-fast.” The high lipid content (around 60%) in mycobacteria’s cell wall makes them acid-fast. SGM require more than 7 days of incubation. Growth of M. avium species can be visualized in both LJ and 7H11 media 5. Colony morphology can be smooth or rough. Biochemical reactions to both niacin and nitrate reduction are negative. Upon growth, colonies can be identified using the MALDI-TOF mass spectrometry 6. However, depending on the database and technology used, reports from the MALDI-TOF may report MAC as M. avium complex or into the individual subspecies. Molecular techniques such as polymerase chain reaction or whole genome sequencing, as well as high-performance liquid chromatography, are required for species identification. Direct detection of nucleic acid in clinical specimens by PCR methods have been reported, although most tests are laboratory-developed and FDA-approved. Molecular technologies typically target the 16S rRNA gene, the 16S-23S internal transcribed spacer (ITS) region or the heat shock protein 65 (hsp65) gene. Prior to PCR, the AccuProbe test was the first commercial molecular assay for identification of mycobacteria by targeting 16S RNA 7. In Japan, an enzyme immunoassay (EIA) kit was used to detect serum IgA antibodies to MAC-specific glycopeptidolipid core antigen. This could be useful for serodiagnosis of pulmonary infections caused by the MAC. This EIA kit’s sensitivity and specificity have been reported to be 54-92% and 72-99%, respectively 8. Other serologic tests are also being investigated.
While this may not aid in the direct detection of MAC infection, a complete blood count (CBC) in DMAC patients frequently shows anemia and, on rare occasions, pancytopenia due to bone marrow suppression caused by the infection, though either leukocytosis or leukopenia may be present. Hypogammaglobulinemia may be another possibility 9. Patients with DMAC typically have elevated transaminase and alkaline phosphatase levels on liver function tests. An HIV test should be performed if pulmonary or disseminated MAC infection is suspected.
MAC is extremely resistant to antituberculosis medications, and a combination of up to six medications is often needed for effective treatment. The preferred medications at the moment are ciprofloxacin, rifabutin, ethambutol, or azithromycin combined with one or more of these other medications 4. For patients with HIV, azithromycin is currently advised as a preventative measure. Of note, preventive treatment of MAC colonization in asymptomatic patients is also not advised. The Clinical and Laboratory Standards Institute (CLSI) recommends performing antimicrobial susceptibility testing using broth microbroth dilution technique. Breakpoints for clarithromycin, amikacin, moxifloxacin, and linezolid are reported 10. Although ethambutol, rifampin, and rifbutin are useful, no official breakpoints are available as there are no strong correlation studies showing the relationship between minimal inhibitory concentrations (MIC) and clinical outcomes.
Figure 1. Acid-fast staining of the bone marrow aspirate revealed many acid-fast bacilli (left, 100X; right, 50X).
2. Miskoff JA, Chaudhri M. Mycobacterium Chimaera: A Rare Presentation. Cureus. 2018;10(6):e2750.
3. Murcia MI, Tortoli E, Menendez MC, Palenque E, Garcia MJ. Mycobacterium colombiense sp. nov., a novel member of the Mycobacterium avium complex and description of MAC-X as a new ITS genetic variant. International journal of systematic and evolutionary microbiology. 2006;56(Pt 9):2049-2054.
4. Kwon YS, Koh WJ, Daley CL. Treatment of Mycobacterium avium Complex Pulmonary Disease. Tuberculosis and respiratory diseases. 2019;82(1):15-26.
5. Hamed KA, Tillotson G. A narrative review of nontuberculous mycobacterial pulmonary disease: microbiology, epidemiology, diagnosis, and management challenges. Expert review of respiratory medicine. 2023:1-16.
6. Body BA, Beard MA, Slechta ES, et al. Evaluation of the Vitek MS v3.0 Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry System for Identification of Mycobacterium and Nocardia Species. Journal of clinical microbiology. 2018;56(6).
7. Ichiyama S, Iinuma Y, Yamori S, Hasegawa Y, Shimokata K, Nakashima N. Mycobacterium growth indicator tube testing in conjunction with the AccuProbe or the AMPLICOR-PCR assay for detecting and identifying mycobacteria from sputum samples. Journal of clinical microbiology. 1997;35(8):2022-2025.
8. Hernandez AG, Brunton AE, Ato M, et al. Use of Anti-Glycopeptidolipid-Core Antibodies Serology for Diagnosis and Monitoring of Mycobacterium avium Complex Pulmonary Disease in the United States. Open forum infectious diseases. 2022;9(11):ofac528.
9. Gordin FM, Cohn DL, Sullam PM, Schoenfelder JR, Wynne BA, Horsburgh CR, Jr. Early manifestations of disseminated Mycobacterium avium complex disease: a prospective evaluation. The Journal of infectious diseases. 1997;176(1):126-132.
10. CLSI. [Performance Standards for Susceptibility Testing of Mycobacteria, Nocardia spp., and Other Aerobic Actinomycetes, 1st ed. CLSI M62. Clinical and Laboratory Standards Institute; 2018
-Dr. Abdelrahman Dabash is currently a PGY-2 pathology resident at George Washington University. He was born in Dakahlia, Egypt, and was raised in Al-Khobar, KSA. He attended the Faculty of Medicine at Cairo University, where he received his doctorate degree. He worked as an NGS analyst for 2 years prior to coming to GWU. His academic interests include Gastrointestinal pathology, hematopathology, and molecular pathology. In his spare time, he enjoys playing soccer, swimming, engaging in outdoor activities, and writing Arabic calligraphy. Dr. Dabash is pursuing AP/CP training.
-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
A 72 year old male presented to UVMMC in July, after being found unconscious and not breathing in his home. The patient presented with swelling of the throat and tongue, which had obstructed his airway. In addition to the swelling, the patient also presented with a hive-like rash along his upper torso and arms along with low blood pressure. The patient was successfully treated by an injection of epinephrine and asked about food allergies, as his clinical presentation was indicative of anaphylaxis. Having declared no food allergies, the patient was asked what he had eaten before the episode, noting that he had a beef burger for dinner hours earlier, which was not unusual for his diet. The attending physician noted the time between the man’s last meal and symptoms of anaphylaxis, which seemingly ruled out a food allergy. The patient was eventually discharged home, with recommendations to monitor his diet and return if symptoms resumed.
Two days later, the patient returned to UVMMC with coughing, shortness of breath, swelling of his tongue and throat, and heartburn. Once again, the patient was treated with injectable epinephrine, which alleviated his symptoms. When asked again about his diet, the man mentioned that hours earlier at dinner he had pork chops, which was also not unusual for his diet. Upon closer examination, a circular rash was observed on the patient’s right shoulder and the patient was tested for Lyme Disease. While awaiting the results of the test, the patient was asked about any exposures to ticks. Upon the mention of tick exposure, the man recalled seeing one a week prior crawling on his arm while he was watering his garden. Insisting that he did not feel a bite and quickly brushed the tick off of his arm, the man described the tick as being brown with a singular white dot on the center of its body. When the Lyme Disease test returned negative, the attending physician ordered a blood test, looking for specific antibodies to alpha-gal. The test returned positive, and the man was diagnosed with Alpha-Gal Syndrome (AGS) from exposure to a Lone Star Tick (Amblyomma americanum) bite. The patient was then referred to an allergist for symptom management.
Figure 1. Image of the rash discovered on the patient’s right shoulder
Lone star ticks (Amblyomma americanum) are aggressive human-biting ticks that actively seek out potential hosts through the use of CO2 trails and vibrational movements.4 This strategy is a distinct behavior when compared to other tick species that commonly employ the ‘ambush strategy’ involving lying in wait for a potential host to pass by.4,5 A complete life cycle for a lone star tick involves three distinct stages, including a larval, nymph and adult stage.3 While the bite of a larval tick is considered less dangerous due to it feeding for the first time and being less likely to have exposure to infected hosts, there is a risk that certain pathogens can be passed from the mother tick to the larvae.4 All three stages of the Lone Star tick’s life cycle require a blood meal from three different hosts, and all stages will feed on humans along with other vertebrate animals.3 These ticks live primarily in areas of woodlands where there is plenty of undergrowth and tall grasses.5
Due to changes in the climate, such as shorter, milder winters and an increased abundance of preferred hosts, the Lone Star tick has increased in both abundance and distribution over the last several decades.3 Despite these concerning trends, these ticks are commonly found throughout the eastern, southeastern, and south-central regions of the United States.3 Because Lyme Disease places such a huge burden on public health populations, the Lone Star tick is often overshadowed in public health messaging by black-legged ticks such as “deer” ticks (Ixodes scapularis) due to their Lyme-carrying abilities.4 In contrast, the Lone Star tick is incapable of transmitting the spirochete that causes Lyme Disease (Borrelia burgdorferi)3, which is a reason why the patient’s blood test was negative for the pathogen in the current case.
Despite being incapable of carrying Lyme Disease, symptoms associated with a Lone Star tick bite may present similarly to that of Lyme Disease including the presence of a rash on the skin.3,4 While similar, this rash is considered distinct from the rash observed in Lyme Disease and has been termed Southern Tick-Associated Rash Illness (STARI).3 While the specific etiologic agent has not yet been identified, the rash is often accompanied by fatigue, headache, fever, and muscle pains and will usually present within seven days of a tick bite.3 While no diagnostic test is available to distinguish STARI from Lyme disease, diagnosis is usually based on symptoms, geographic location, possibility of a tick bite, and the presentation of the rash which is typically a red circle expanding to around 8cm in diameter.3
Lone Star ticks can transmit a variety of bacterial and viral pathogens, but they are most commonly associated with Alpha-Gal Syndrome (AGS).2,3,4,5 Alpha-Gal refers to the sugar molecule galactose-alpha 1,3-galactose, which is commonly found in most mammals except people, fish, reptiles, and birds.2 The sugar molecule is found in meats (pork, beef, rabbit, lamb, venison, etc.), as well as in mammalian products such as gelatin, cow’s milk, or milk products.2 Lone Star ticks transmit this sugar to humans by feeding on hosts and maintaining trace amounts of alpha-gal within their salivary glands, which is then injected into the next host.2,4 In humans, the immune system reacts to alpha-gal in the bloodstream similarly to a foreign invader, initiating an IgE-mediated allergic response.4 Symptoms will often vary between each individual but can include hives, nausea, vomiting, heartburn, dizziness or fainting, and anaphylaxis, among many other symptoms.2,4
It is estimated that between 2010 and 2022, more than 110,000 people were suspected of having AGS, and diagnosis is usually confirmed by blood tests which look for specific antibodies to the sugar.2 Interestingly, not every exposure to alpha-gal will result in an allergic reaction, and unlike food allergies where exposure can result in immediate reaction symptoms, it could take up to several hours after ingestion of an animal product containing alpha-gal for symptoms to appear in AGS patients.4 Unfortunately, there is no treatment for AGS, but patients are typically managed by an allergist with recommendations of carrying an injectable epinephrine device, avoiding foods containing alpha-gal, taking antihistamines as needed, and monitoring or adjusting other medications which may be manufactured using gelatin capsules.2,4
4 Kennedy, A. C., BCE1, & Marshall, E. (2021). Lone Star Ticks (Amblyomma americanum):: An Emerging Threat in Delaware. Delaware journal of public health, 7(1), 66–71. https://doi.org/10.32481/djph.2021.01.013
-Maggie King is a Masters student in the Department of Pathology and Laboratory Medicine at the University of Vermont.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
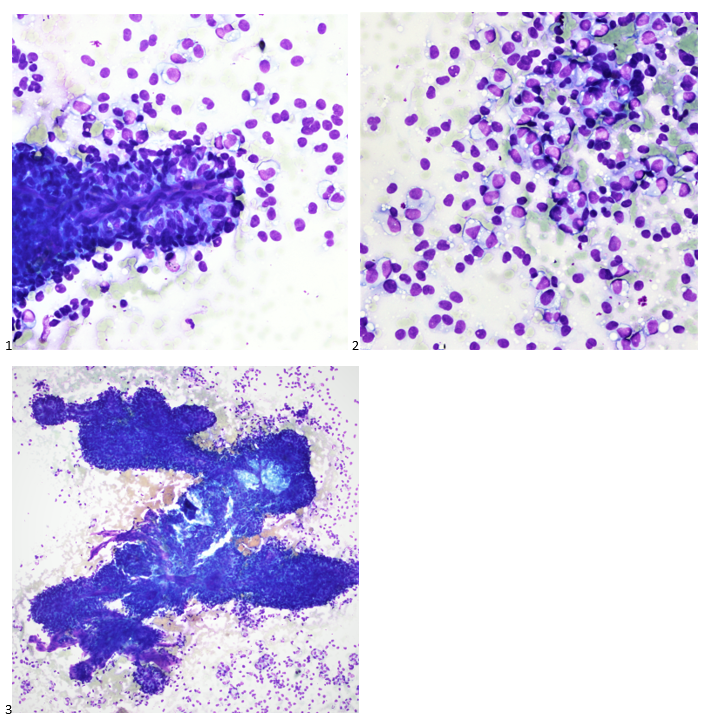
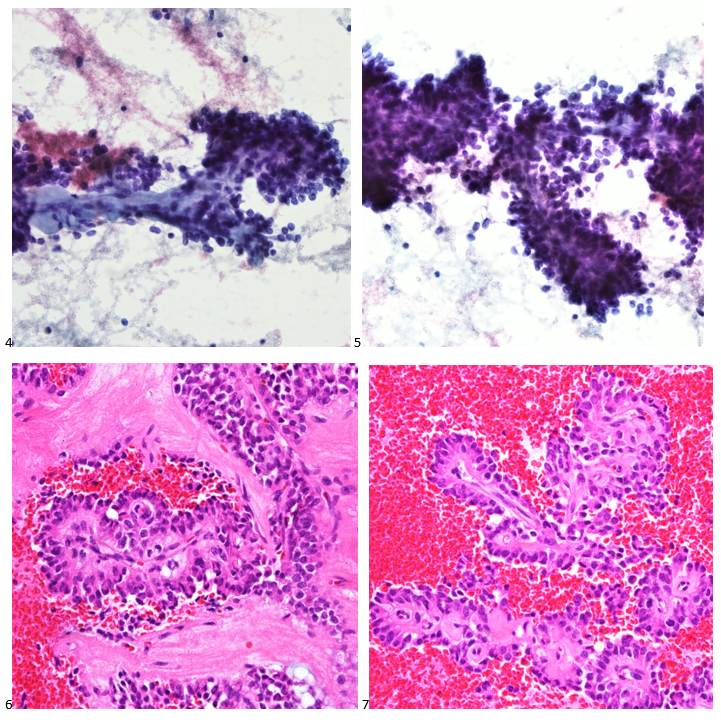
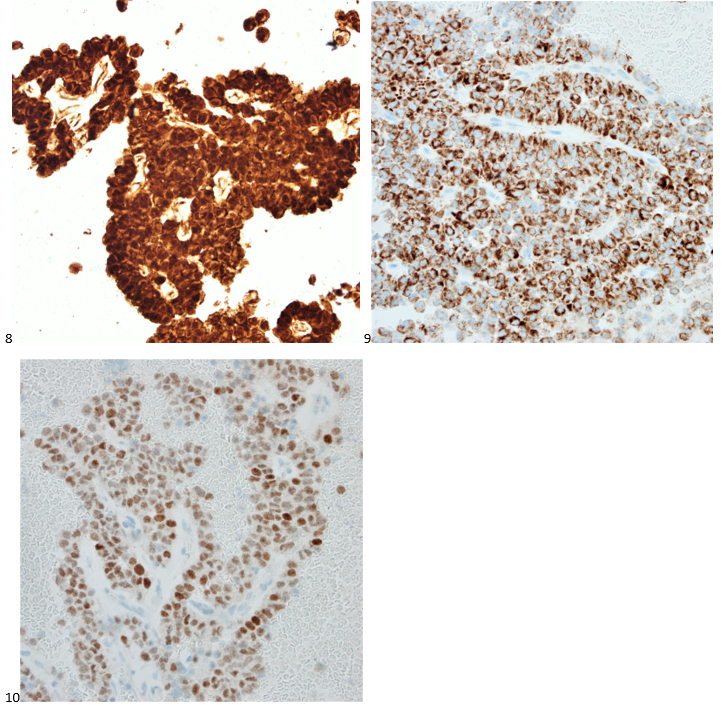
A 20 year old female patient referred herself to a surgical oncologist specializing in sarcomas after she presented to an outside hospital for a sudden onset of epigastric pain. The patient also reported a one-year history of decreased appetite without nausea, vomiting, or weight loss. The outside institution performed an abdominal ultrasound and identified a large nonvascular heterogenous masslike lesion in the left upper quadrant not definitively associated with the spleen or kidney. The mass measured 12.1 x 9.9 x 10.7 cm. The radiologist’s overall impression was a hematoma; however, a CT scan with contrast was recommended to further classify the lesion. Instead, an MRI was performed, and the same radiologist described the lesion as having a thick irregular enhancing rind with enhancing septations and central necrosis. With the lesion appearing distinct from adjacent organs, a retroperitoneal sarcoma was posited on imaging. Reviewing the outside imaging and clinical history, the surgical oncologist referred the patient to interventional radiology for an ultrasound-guided biopsy of the left-sided retroperitoneal mass.
When the cytologist arrived in the procedure room for the time-out, the radiologist informed her of the surgical oncologist’s and outside radiologist’s opinions of a retroperitoneal sarcoma. A 17-gauge coaxial needle was advanced into the peripheral and non-necrotic aspect of the retroperitoneal mass, and multiple 22-gauge fine needle aspirations were obtained and handed to the cytologist. She prepared two air-dried smears and two alcohol-fixed slides. The air-dried smears were stained in our Diff-Quik (DQ) set-up and deemed adequate. The pathologist’s immediate cytologic evaluation was “tumor cells present.”
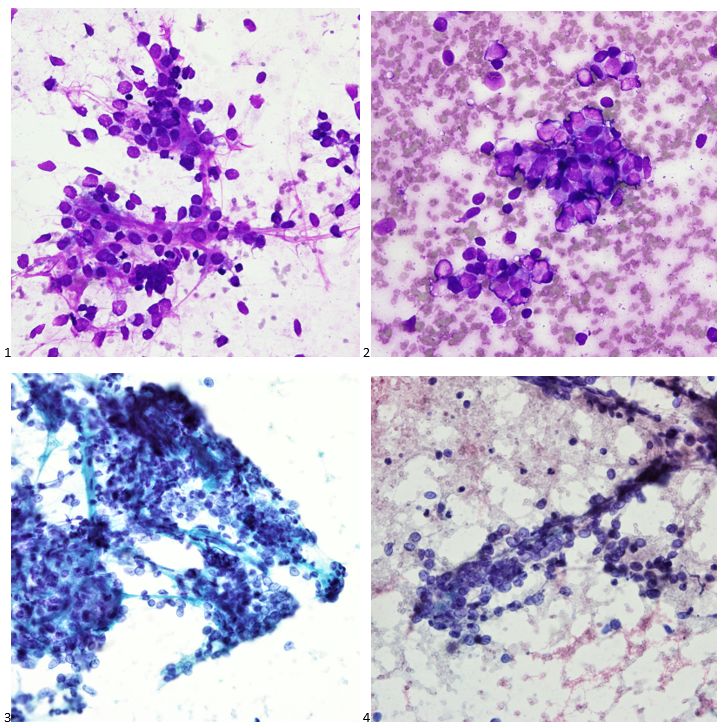
The following morning, the cytologist primary screened the Papanicolaou-stained slides and H&E-stained cell block sections in addition to the DQ smears, with the former preparations presented below.
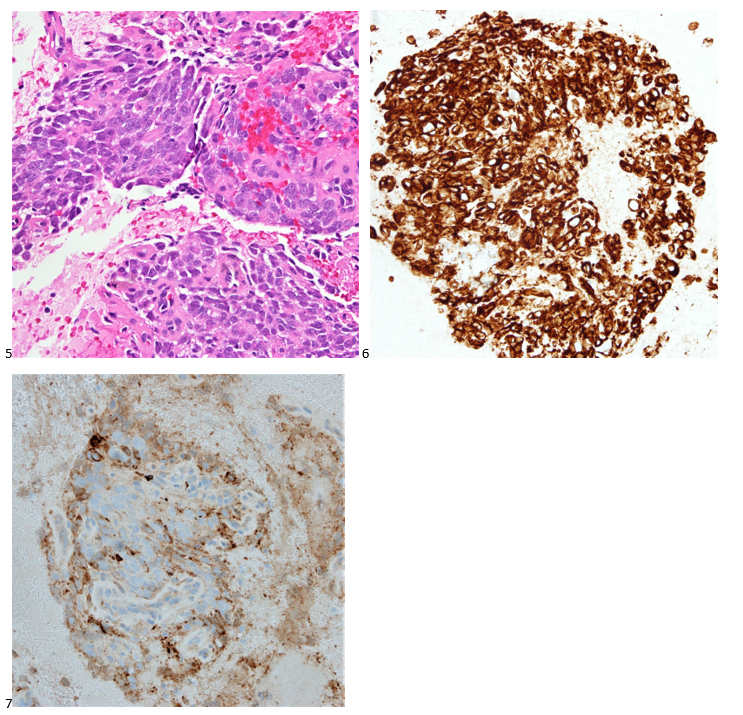
The cytologist entered her results as positive for malignant cells with a note of “atypical cells in papillary fragments” and gave the case to the pathologist for the final interpretation. The pathologist reviewed the slides prior to ordering immunostains. He paused and thought, “there’s something about the morphology and her age… it just doesn’t make sense for this to be a retroperitoneal sarcoma. It doesn’t look like a sarcoma. The cells are just too round or ovoid, bland, and poorly cohesive, and the fibrovascular cores – I just don’t think this is a sarcoma. Maybe a melanoma? Or some type of renal tumor? The cytoplasmic vacuolization could suggest this, but the mass is distinct from the kidney, so it can’t be. The nuclear grooves are intriguing, almost like a papillary thyroid carcinoma. A neuroendocrine tumor is also possible, the delicate papillary fronds though… Hmm. But where would it be originating from? How could this be distinct from other organs in the abdominal cavity?” He hemmed and hawed, glancing over our list of in-house immunostains. With only nine pre-cut unstained sections associated with the three H&E cell block levels, the pathologist ordered additional unstained recuts. He knew this was going to be a challenge due to the discrepancy between the clinical history and the morphology.
With proper positive and negative controls, the tumor cells show positive staining for AE1/AE3, Cam 5.2, vimentin, CD99 (dot-like), CD56, beta catenin (nuclear), PR, AMACR, and SOX11, while negative staining for CK7, CK20, PAX-8, RCC, chromogranin, synaptophysin, GATA-3, EMA, GFAP, S100, calretinin, WT-1, E-cadherin, and p53 (wild type pattern). The proliferative index by Ki-67 is low at <1%.
The combination of morphology with the extensive immunoprofile of the tumor is consistent with solid pseudopapillary neoplasm (SPN) of the pancreas.
Had there been any mention of the tumor involving or replacing the pancreas, this diagnosis and workup would have been much more straightforward. SPNs, albeit rare, account for 30% of tumors in women within their third or fourth decade of life.1 This patient presented with the most common SPN symptoms of abdominal pain and early satiety, but the mass appearing extrapancreatic on imaging posed a diagnostic challenge, as extrapancreatic SPNs are rare.2-3 Fortunately, SPNs are low-grade malignant neoplasms that respond well to surgical resection, and this patient is doing just fine after her distal pancreatectomy. In this case, both the patient and our pathologist listened to their guts with the patient pursuing advanced medical care for something much more complicated than a hematoma and the pathologist relying on his morphology expertise despite an odd clinical presentation.
References
La Rosa S, Bongiovanni M. Pancreatic solid pseudopapillary neoplasm: key pathologic and genetic features. Archives of Pathology & Laboratory Medicine. 2020;144(7):829-837. doi:10.5858/arpa.2019-0473-ra
Dinarvand P, Lai J. Solid pseudopapillary neoplasm of the pancreas: a rare entity with unique features. Archives of Pathology & Laboratory Medicine. 2017;141(7):990-995. doi:10.5858/arpa.2016-0322-rs
Cheuk W, Beavon I, Chui D, Chan JKC. Extrapancreatic solid pseudopapillary neoplasm. International Journal of Gynecological Pathology. 2011;30(6):539-543. doi:10.1097/pgp.0b013e31821724fb
-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
A 75 year old man came to the Emergency Room because of intractable hiccups. He had a medical history of esophagitis, gastroesophageal reflux disease, gastric metaplasia diagnosed during a previous esophago-gastroduodenoscopy (EGD), and a significant episode of hiccups for several years. His esophagogastroduodenoscopy revealed diffuse edema and erythema on the duodenal mucosa. Histopathological examination of the duodenal biopsies (Figures 1-3) showed the presence of Strongyloides stercoralis within a few crypts of the duodenum, and adjacent eosinophil-rich inflammatory infiltrate within the mucosa. These findings provided an incidental finding of the parasite’s presence in the duodenal mucosa.
Figure 1. H&E stain of the biopsy at 10X Figure 2. H&E stain of the biopsy at 400X Figure 3. H&E stain of the biopsy at 400X
Discussion
Strongyloidiasis is a parasitic infection caused by the nematode Strongyloides – most commonly S. stercoralis. While it is commonly seen in tropical and subtropical regions, cases can also occur in temperate climates. Notably, our patient had a recent travel history to Jamaica, a known endemic region for Strongyloides infection.
The life cycle of Strongyloides stercoralis involves both free-living and parasitic stages. The infectious filariform larvae penetrate the human skin typically after contact with contaminated soil or exposure to infected fecal matter. Subsequently, they migrate to the lungs through the bloodstream, and eventually reach the small intestine, where they mature into adult worms. The adult worms reside in the duodenal and proximal jejunal mucosa, reproducing asexually by parthenogenesis. Some of the eggs hatch within the intestine, releasing rhabditiform larvae into the feces. It causes autoinfection by penetrating the intestinal wall or the perianal skin area.
The diagnosis of Strongyloides is typically accomplished by morphologic identification of larvae in the stool, duodenal aspirate, or sputum in disseminated cases. Strongyloides serologic testing is often performed in transplant patients who have a pertinent demographic and clinical history of potential exposure. The presence of eggs is rarely observed in the stool; therefore, microscopic examination of stool samples may have a lower sensitivity in uncomplicated infection with a low organism burden. In our case, stool samples were not collected for evaluation. Hyper-infection syndromes associated with disseminated Strongyloides could present as subclinical infection in patients under immunosuppression. As the larvae invade other organs, such as CNS, lungs, and blood stream, intestinal flora from the GI tract is carried along with the larvae, which causes super-infections, such as bacteremia and meningitis.
No FDA-cleared molecular testing is available for Strongyloides while some reference laboratories may offer laboratory-developed-tests. Therefore, the laboratory diagnosis frequently relies on the morphologic identification of the filariform larvae or eggs from clinical samples. In our case, the histopathological examination of the duodenal biopsies that were obtained to evaluate persistent hiccups revealed a significant eosinophil-rich inflammatory infiltrate within the mucosa, along with the presence of the larvae within the crypts. While hiccups can be due to various etiologies, including gastrointestinal disturbances and certain medications, and may not be directly related to parasitic infections, the diagnosis of Strongyloides in this case was purely incidental.
De la Cruz Mayhua, Juan Carlos, and Bisharah Rizvi. “Strongyloides Hyperinfection Causing Gastrointestinal Bleeding and Bacteremia in an Immunocompromised Patient.” Cureus, 24 June 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC8310433/.
-Inas Mukhtar, MD, is from Sudan and graduated medical school from University of Khartoum and started a pathology residency in Sudan before applying here to the US. She is currently PGY-2 at Montefiore Medical Center. Her hobbies include watching documentaries and spending time with friends and family.
-Phyu Thwe, Ph.D, D(ABMM), MLS(ASCP)CM is Associate Director of Infectious Disease Testing Laboratory at Montefiore Medical Center, Bronx, NY. She completed her medical and public health microbiology fellowship in University of Texas Medical Branch (UTMB), Galveston, TX. Her interests includes appropriate test utilization, diagnostic stewardship, development of molecular infectious disease testing, and extrapulmonary tuberculosis.
Working in Hematology, I have learned that things aren’t always black and white. With about 80-85% of our CBC’s autovalidating, it’s those other “problem child” specimens that can give us a challenge. When we get one of these tricky specimens, it’s time to put on our detective hats and investigate what is going on.
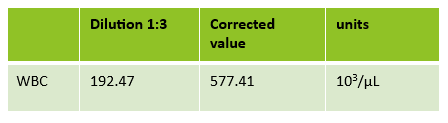
This patient was a 65-year-old female with Chronic Lymphocytic Leukemia (CLL). WBC and RBCs are counted on our analyzer by impedance, which sorts cells by size. When we ran this sample, we noticed a few things right away. See results below in Figure 1.
Figure 1. Original CBC results with Instrument Flags
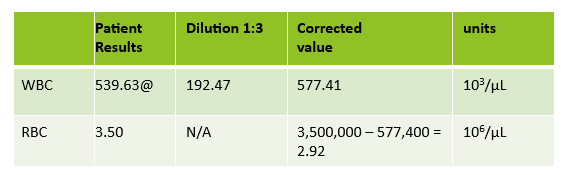
The first thing I notice on this specimen is the @ next to the WBC. This indicates that the count is over linearity and was confirmed by dilution. The corrected WBC was 577 x 103/mL. See Figure 2.
Figure 2. 1:3 dilution results for WBC. 192.47 x 3 = 577.41 x 103/μL
Extreme leukocytosis may interfere with the RBC, HGB, HCT and MCV determinations. The degree of RBC interference depends on the number and size of WBCs present. WBC and RBC are counted using impedance technology. In impedance counting, the RBC count is done first by passing the sample though the aperture in the RBC/platelet channel. This count is actually the sum of both RBC and WBC counts. Then, the RBCS are lysed and the WBCs are counted in the WBC channel. Normally, the WBC count has very little, if any, effect on the reported RBC count. Normal RBC counts are 4-6 million/μL. Normal WBC counts are a fraction of this, at about 5-10,000/μL. If the the RBC count is 3.50 x 106/μL and the analyzer includes 10,000 WBCs in the count, this only changes the RBC to 3.51 x 106/μL. (3,500,000 + 10,000 = 3,510,000). Because WBC counts are so much lower than RBC counts, even if a WBC count is 100,000, the effect on the RBC count is clinically insignificant. (3,500,000 + 100,000= 3,600,000 = 3.60 x 106/μL) However, in this patient, the WBC count was 577,000/μL. After reviewing the smear and confirming the WBC count with a WBC estimate, we corrected the RBC count, by subtracting the WBC from the RBC. As you can see in figure 3 below, the extreme leukocytosis did affect the RBC count.
Figure 3. Corrected RBC count. Subtract the WBC count from the RBC count. Corrected RBC (cRBC) = RBC (x 106/μL) – WBC (x 103/μL)
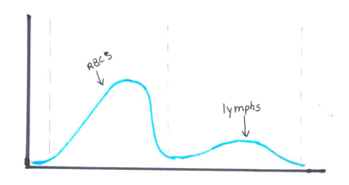
So, how does this affect the hematocrit? The next thing noticed right away is that the Hgb and Hct don’t follow the “rules of 3”. Now, we know that these rules really only hold true for normocytic, normochromic RBCS, but extreme leukocytosis can interfere with Hct determination. A Hgb of 9.2 g/dL and Hct 39.4% doesn’t look ‘right’. We have just corrected the RBC count, and now we need to ask ourselves how this can affect the Hct. The hematocrit is the packed cell volume, or the % of red blood cells per total volume of the sample. Since we now know that the RBC count is 2.92 x 106/μL, not 3.50 x 106/μL, we can correct the hematocrit. If you have a hematocrit centrifuge in your laboratory, a spun hematocrit can be used to determine the corrected hematocrit. After correcting the Hct, you must also correct the MCV using the following formula.
Corrected MCV (cMCV) = HCT(%) x 10/cRBC
Another option for resolving interferences and correcting the Hct for extreme leukocytosis is using the clues that the RBC histogram gives us. We know the RBC count needed correcting, and we subtracted the WBC to get the corrected RBC. This sample had multiple flags. One of them was “Dimorphic population”. This indicates two populations of RBCs in the sample. Since we know a considerable number of WBCs were counted in the RBC chamber, this would account for the dimorphic population. A dimorphic population on histogram looks like what I call a ‘double humped camel’. In this case, the patient’s RBCs are the first, smaller population and the lymphocytes of this CLL patient are the 2nd larger population. See Figure 4.
Figure 4. Example of a dimorphic RBC histogram.
Another option for recalculating the MCV is using the information in the service tab of your analyzer. Note that the results from the service tab are not FDA approved, and therefore not directly reportable, so must be confirmed first. If using values from the service tab, the spun hematocrit and calculations can be used as a check. The service tab displays the MCV of these 2 populations. These are listed as the MCV of the small population, S-MCV, and the MCV of the large cell population, L-MCV. Using the small MCV (sMCV) value and the corrected RBC (cRBC), we can back calculate the Hct using the following formula.
Corrected Hct (cHct) (%) = (sMCV x cRBC)/10
For this sample:
S-MCV = 105.1
L-MCV= 215.4
(cHct) (%) = 105.1 x 2.92/10 = 30.7 %
Hgb is another parameter that may be affected by extreme leukocytosis. Turbidity may be present in the diluted and lysed sample when reading the Hgb. This sample did not give us a Hgb turbidity flag, but because of the high WBC, the Hgb was confirmed using a diluted sample. The sample was diluted 1:3 with the analyzer diluent. Results were multiplied by the dilution factor. Lastly, when performing Hgb corrections (and in this case, also the RBC corrections) you must also recalculate the MCH and MCHC using the corrected values. Figure 5 shows these corrected values.
MCH (pg)= (cHgb/cRBC) x 10
MCHC (g/dL) =(cHgb/cHct) x 100
Figure 5. Corrected CBC results
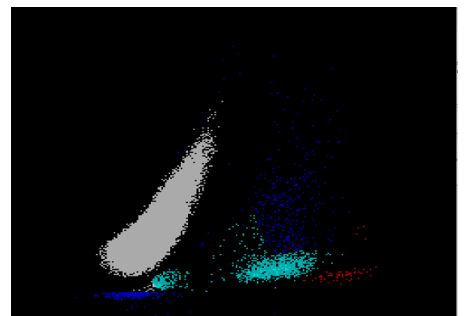
We can breathe a sigh of relief that we finally have accurate and reliable results for the CBC. But what about the differential? This big ugly grey mess seen in Figure 6 on the differential scattergram indicates a very abnormal scattergram. This is telling us that there is no separation between the types of cells. There were multiple flags for WBC abnormal scattergram, leukocytosis, lymphocytosis, and a flag for dimorphic RBC populations. These flags are all telling us not to accept the instrument results. In these cases, we want to review the smear, do a WBC estimate, and perform a manual differential, examining the differential carefully to look for any abnormalities. The differential had many lymphocytes and smudge cells. An albumin smear was made to resolve the smudge cells and a manual differential was performed.
Figure 6. WDF Scattergram
I’ll admit that this type of specimen is not something we encounter every day (thankfully). But I thought it a very interesting example of a spurious results on many levels. These challenges are some of my favorite things about working in Hematology. Using autovalidation is a great tool in the laboratory to help workflow. With about 85% of specimens autovalidating, this allows us to spend time on these tricky specimens. And this tricky specimen was an epic one! We had CBCs on this patient several days in a row. Unfortunately, some of her results were simply repeated and reported. Some WBC results over linearity were reported without dilution. Other parameters were not corrected. This gives inconsistent and confusing results to the physicians and is not beneficial to the patient. Because of the inconsistencies, we issued a couple corrected reports which can be very time consuming. Sometimes we may not have the answers and can’t resolve a problem. If a specimen cannot be resolved, it is always better to report what you can and use ‘not reported’ or ‘not measured’ for any results that are not available. It’s better to report the good results that you have than to report junk that physicians can’t rely on. I often say that simply repeating a sample and reporting results if they match is not sufficient. We need to investigate spurious results so that we may report the best quality results possible for every patient.
References
Gulati G, Uppal G, Gong J. Unreliable Automated Complete Blood Count Results: Causes, Recognition, and Resolution. Ann Lab Med. 2022 Sep 1;42(5):515-530. doi: 10.3343/alm.2022.42.5.515. PMID: 35470271; PMCID: PMC9057813.
Sysmex USA. XN-Series Flagging Interpretation Guide. Document Number: 1166-LSS, Rev. 6, March 2021
Zandcki, M. et al. Spurious counts and spurious results on haematology analysers: a review. Part II: white blood cells, red blood cells, haemoglobin, red cell indicies and reticulocytes. International Journal of Laboratory Hematology. 09January 2007.
-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
A 36 year old male was referred to gastroenterology after presenting to the emergency room for hematemesis and severe fatigue. He was pale and tachycardic, and the CBC showed a hemoglobin of 4.5. An esophagastroduodenoscopy (EGD) at the time demonstrated erosive esophagitis with a visible vessel and was treated with a PPI. A repeat scope the following month no longer demonstrated a vessel but identified a 10 cm ulcerative gastric cardia mass at the GE junction. Forcep biopsies showed a gastric ulcer with granulation tissue, and the stains performed yielded results that were not consistent with carcinoma or lymphoma; however, the biopsy material was limited, and the patient was referred to our GI clinic for further workup.
The interventional gastroenterologist requested cytology be present for the patient’s endoscopic ultrasound to ensure an adequate specimen was obtained for a definitive diagnosis. During the rapid onsite evaluation (ROSE), we determined the Diff-Quik smear was adequate, and the pathologist could confidently suggest that tumor cells were present. We collected additional FNA passes in our cell block tube to run ancillary studies.
The following morning, all we could make of the case was that it was a poorly-differentiated malignant neoplasm with spindle and epithelioid features. The cytoplasm was minimal and fairly wispy while the nuclei were hypochromatic and fragile with nuclear grooves and nucleoli. On the Diff-Quik smears, the cytoplasm looked blue, which pointed us in the direction of possibly lymphoma or neuroendocrine, but the clustering made me favor neuroendocrine. With the pap-stained smears, were torn between carcinoma and a neuroendocrine tumor, maybe even an epithelioid GIST, albeit an odd location. And of course, there’s always the differential of melanoma, the great mimicker. Off to IHC we go!
When our immunostains were delivered later that afternoon, our pathologist came up to me and said, “I got it! I know what it is!” Ecstatic, I replied, “What is it? Lymphoma? Carcinoma? GIST? MELANOMA?” “No, it’s a WEIRDOMA! Nothing is staining positive. No epithelial markers, no definitive lymphoid markers… nothing. It’s a weird case. I have to run additional stains.”
Back to the drawing board and 20 additional recut sections later, more immunostains were ordered and a mixed profile led us down a more confusing path. The tumor cells show positive staining for vimentin, CD56, and CD10 (focal), and negative staining for AE1/AE3, Cam5.2, CK7, desmin, SMA, HHF35, CD34, CD117, DOG-1, S100, SOX-10, synaptophysin, SALL4, CD45, CD68, and CD21. Proliferative index by Ki-67 was approximately 35%. The morphology and immunoprofile of the tumor were highly unusual, suggesting a mesenchymal neoplasm, possibly a sarcoma.
The concurrent forcep biopsies demonstrated rare atypical cells that were difficult to classify due to the limited number of cells, the non-specific morphology, and the following non-specific immunophenotype: positive staining for CD99, partial positive staining for D2-40 and NSE, and focal or weak positive staining for Cam5.2, while negative for AE1/AE3, CK7, EMA, S100, CD31, desmin, PAX8, BCL2, and myogen. The biopsy tissue consisted of predominantly ulcerative tissue and a fragment of squamous mucosa with a lamina propria infiltrate of atypical cells with spindle and epithelioid morphology.
Due to the FNA cell block consisting of 80% tumor compared to the limited forcep biopsy tissue, we sent FFPE cell block sections for RNA fusion studies to help us further classify the tumor. An EWSR1::ERG (in-frame) rsa(22;21)(q12.2;q22.2) gene fusion was detected in the tissue sample, which has been reported in extraskeletal Ewing sarcoma.
Stomach, GE Junction, EUS-FNA Final Diagnosis: Ewing Sarcoma
Fortunately, the patient’s PET scan did not demonstrate any evidence of metastatic disease, and the patient along with his care team decided to pursue systemic therapy as these tumors tend to be chemosensitive. The need for radiation therapy will be reviewed depending on the tumor’s response to systemic therapy. A strange presentation, this visceral Ewing sarcoma, and a reason why immunostains and molecular profiling are so important to rendering a definitive diagnosis. In our study set files, however, it will forever be dubbed my favorite weirdoma.
-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
A 74 year old male presented to UVMMC for a routine sputum culture at the adult cystic fibrosis (CF) clinic. At this visit, there were no pulmonary complaints, but chest imaging indicated scarring and atelectasis of the right upper lung and left mid lung. The imaging did not show signs of pulmonary infection.
The patient’s initial diagnosis of CF occurred at age 69 after a history of recurrent respiratory infections, bronchiectasis, and infertility. An elevated sweat chloride confirmed a CF diagnosis and subsequent genetic testing showed heterozygosity for 2 disease-causing CFTR mutations: p. Leu206Trp and p. Phe508del. Additional relevant medical history includes a history of smoking and ongoing pancreatic issues likely related to CF. The patient has been prescribed elexacaftor/texacaftor/ivacaftor which seems to be improving his pulmonary symptoms, as well as supplemental pancreatic enzymes which have moderately improved his pancreatic symptoms. Routine sputum cultures are often performed in CF patients to monitor treatment and disease progression, as well as detect any possible latent infections.6 A culture from this same patient in 2022 indicated an infection with Pseudomonas fluorescens, highlighting the importance of routine disease monitoring in CF patients.
Laboratory Workup
The sputum sample taken from the patient was routinely processed and planted to blood, chocolate, MacConkey, CNA, and Burkholderia cepacian agars. Growth from both the blood agar plate and the chocolate agar plate contained an organism with mucoid morphology, in addition to normal oropharyngeal flora. After subbing out these mucoid colonies, organism growth was observed on both a blood agar plate and a MacConkey medium plate. Growth from the MacConkey agar plate indicated the organism was a non-lactose fermenter, as observed in the un-pigmented colonies and the agar itself remaining a pink color.3 The mucoid organism was determined to be a mucoid strain of Pseudomonas aeruginosa from MALDI-ToF.
Figure 1. A blood agar plate. This plate shows growth of normal oropharyngeal flora, while also containing a bacterium of mucoid morphology. There are numerous colors, colony morphologies, and organisms present on the plate.Figure 2. A chocolate agar plate displaying mixed microbial growth. Some colonies are yellow in color with poorly defined margins, while other colonies are white with clearly defined margins. It was determined that the majority of the colonies present on this plate are normal oropharyngeal flora.Figure 3. Blood agar plate with mucoid morphological growth which was isolated from the plate shown in Figure 1.Figure 4. MacConkey medium growing bacteria with mucoid morphology. The bacteria itself remains an un-pigmented, brownish color while the agar itself had stayed pink. Both the colony color and agar color are indicative that the organism is not a lactose fermenter.3
Discussion
Cystic fibrosis (CF) is an autosomal recessive disease with the potential to affect multiple organ systems including the respiratory, digestive, and reproductive systems.7 The primary cause for this disease stems from mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene, of which more than two thousand different mutations have been described.1 In healthy individuals, this gene is responsible for the production of a protein that transports salts across different bodily tissues, yet mutated versions of this gene produce proteins that are absent or dysfunctional, and thus cannot promote salt transport and water movement as efficiently.2 The various mutations of the CFTR gene can result in numerous types of clinical presentations, but these mutations are most often observed to impact mucus viscosity with thick, sticky mucous along with chronic respiratory infections considered a hallmark of this disease.7 Further, decades of research have described additional manifestations of CF, including infertility, chronic sinusitis, and pancreatic damage, as well as an increased risk for dehydration.2
The most commonly performed diagnostic test for CF patients includes a sweat chloride test, for which a sweat chloride concentration above 60 mmol/L is indicative of a CF diagnosis and results directly from the loss of function of the CFTR proteins.1 Since the first descriptions of CF in 1935,1 newborn screening programs have been implemented with the hopes of catching potential cases early and improving prognoses. The newborn test screenings are often focused on the detection of immunoreactive trypsinogen in the blood, as the levels of this chemical are often elevated in patients with CF.1
Further, DNA analysis has proven to be an extremely useful tool in the diagnosis of CF patients, but these analyses are limited to the detection of only the most common mutations and can misdiagnose some of the rare variants of the disease.7 Additionally, because there is a wide range of disease-causing genotypes resulting in CF, some patients may exhibit a late onset of symptoms while still having two CFTR mutations, accounting for the increase of diagnoses made during adulthood.1 This would explain why the patient, in this case, may have been diagnosed so late in life; with two separate gene mutations, the patient may not have exhibited the classical symptoms of CF earlier in life.
Pseudomonas aeruginosa is a common pathogen found in CF patients and contributes significantly to patient morbidity and mortality.4P. aeruginosa, upon infection of the lung, promotes the accelerated decline of pulmonary function in CF patients and has been shown to exhibit significant resistance to both the innate immune system and antibiotics through the expression of specific virulence factors.5 Because CF patients are susceptible to chronic lung infections, repeat treatment with antibiotics has also been shown to promote adaptive mutations to P. aeruginosa, making this pathogen a particularly dangerous organism for CF patients.5 The versatility of the organism makes it capable of causing both acute and chronic infections, and the persistence of P. aeruginosa within CF patient airways into adulthood can be explained by the complex relationship between the organism’s pathogen traits and various host factors.4
Because P. aeruginosa has a reputation for being especially resistant to antibiotics, it is especially difficult to treat in CF patients who are routinely treated for chronic infections. The best treatment course would be to conduct an antibiotic resistance panel from the sputum culture sample to determine which of the available antibiotics might have the greatest treatment response against the bacteria.
References
1 De Boeck K. (2020). Cystic fibrosis in the year 2020: A disease with a new face. Acta paediatrica (Oslo, Norway : 1992), 109(5), 893–899. https://doi.org/10.1111/apa.15155
3 Jung, B., Hoilat, G.J., (2022, September) MacConkey Medium. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Accessed on September 26th, 2023, from: https://www.ncbi.nlm.nih.gov/books/NBK557394/
4 Jurado-Martín, I., Sainz-Mejías, M., & McClean, S. (2021). Pseudomonas aeruginosa: An Audacious Pathogen with an Adaptable Arsenal of Virulence Factors. International journal of molecular sciences, 22(6), 3128. https://doi.org/10.3390/ijms22063128
5 Malhotra, S., Hayes, D., Jr, & Wozniak, D. J. (2019). Cystic Fibrosis and Pseudomonas aeruginosa: the Host-Microbe Interface. Clinical microbiology reviews, 32(3), e00138-18. https://doi.org/10.1128/CMR.00138-18
6 National Guideline Alliance (UK). Cystic Fibrosis: Diagnosis and management. London: National Institute for Health and Care Excellence (NICE); 2017 Oct 25. (NICE Guideline, No. 78.) 9, Pulmonary monitoring, assessment and management. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535669/
7 Radlović N. (2012). Cystic fibrosis. Srpski arhiv za celokupno lekarstvo, 140(3-4), 244–249. Accessed on September 28th, 2023, from: https://pubmed.ncbi.nlm.nih.gov/22650116/
-Maggie King is a Masters Student in the Department of Pathology and Laboratory Medicine at the University of Vermont Larner College of Medicine.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.