As a clinical instructor and lead cytologist at my institution, I like to remind our newer cytologists and cytology students of the importance of being prepared for FNA biopsies so they develop good habits or best practices as they become more experienced. This level of preparation helps to create a culture of ongoing learning and improvement, which is necessary for the laboratory. In my experience, I’ve met some cytologists who prefer to go into a case blind, with the mindset that knowing the patient’s clinical history in advance muddies their knowledge, skills, and abilities, limiting their mindset by excluding the possibility of other diagnoses. While diving into the unknown might seem exciting, it is also a hindrance and could result in errors, especially when the clinical history helps us triage the patient’s sample. For example, knowing that the patient has a history of lymphoma or that the presentation state includes bulky lymphadenopathy prompts us to collect additional needle passes to send for flow cytometry analysis. Another concern is not knowing whether the patient has a history of breast, gastric, or esophageal cancer, and consequently processing the specimen routinely, which may result in an extended cold ischemic time. This delay in fixation along with insufficient formalin fixation can yield false negatives on ER/PR IHC in breast cancers and HER2 FISH in breast, gastric, and esophageal cancers, which could restrict the use of hormone therapies, such as tamoxifen and aromatase inhibitors for hormone receptor-positive (HR+) cancers, or trastuzumab for HER2+ cancers. I cannot overemphasize the importance of familiarizing yourself with clinical history and communicating case specifics while you act as a mediator between clinician and pathologist.
Whether the clinical history impacts the pre-analytical phase, such as specimen collection (limiting cold ischemic time or collecting additional needle passes for ancillary studies) or the analytical phase, as such processing (formalin fixation) and diagnosis (selecting an appropriate immunoprofile), we must remain vigilant and proactive in laboratory medicine. In this case, knowing the patient’s clinical history was of the utmost significance as it helped to reduce the number of immunostains and ancillary studies necessary to make the diagnosis. Using morphologic criteria in tandem with the patient’s clinical history narrowed the differential diagnoses to just two possible types of cancer, presented below.
A 59 year old male patient presented to the emergency room after an automobile accident. On imaging, the X-ray and CT scan identified a left humerus mass and fracture, and bloodwork was performed. His medical record was sparse and uneventful with no recent visits or encounters. To build a more comprehensive wellness profile and prepare for surgery, he was also offered a one-time screening for Hepatitis C, as an adult who was born between 1945 and 1965.
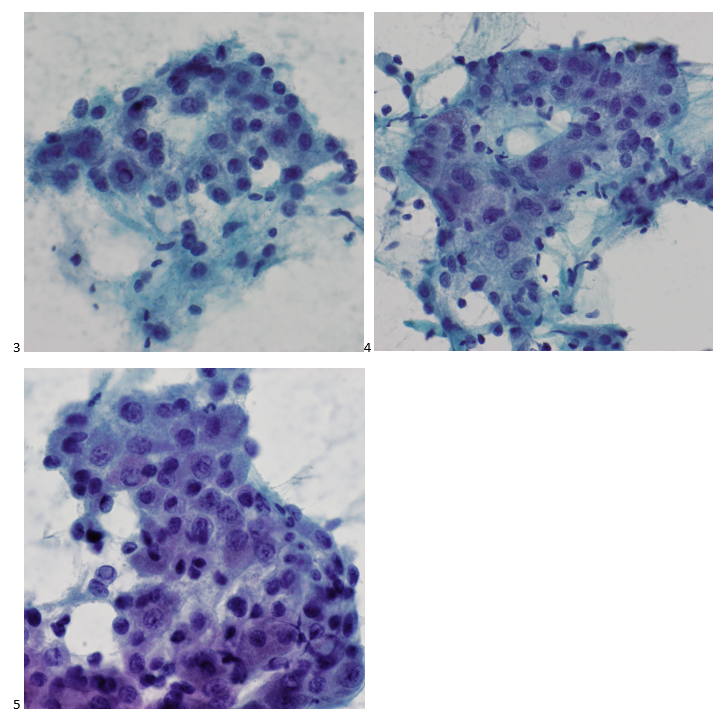
The left humerus mass was biopsied via CT-scan guidance and two passes were obtained. The Diff-Quik stained smears demonstrate large polygonal cells, some with abundant, granular cytoplasm and some isolated cells with naked nuclei. Vessels also appear to traverse some of the cell groups.
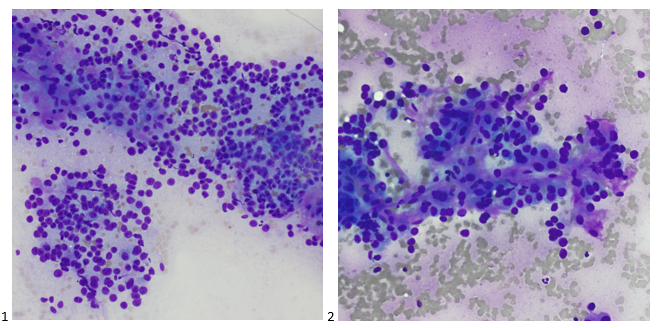
The Pap-stained smears also demonstrate polygonal cells with granular cytoplasm, nuclei with coarse chromatin, and prominent nucleoli. An interesting feature frequently identified in this case is the intranuclear inclusions, and in hindsight, a focus on these may have further reduced the number of immunostains performed.
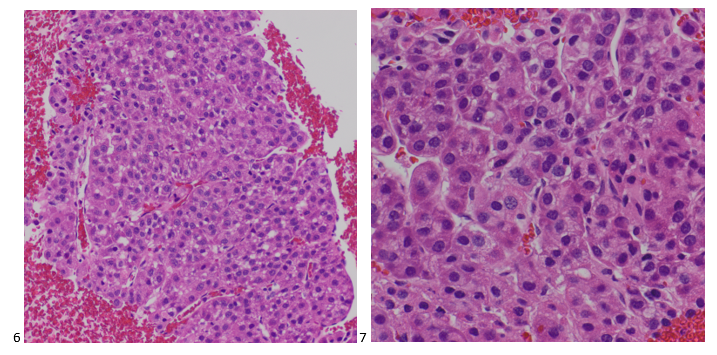
The H&E-stained cell block sections show trabeculae with endothelial wrapping around the cell cords. While renal cell carcinoma was listed as a differential diagnosis due to its telltale oncocytic cytoplasm and vascularity, hepatocellular carcinoma was favored.
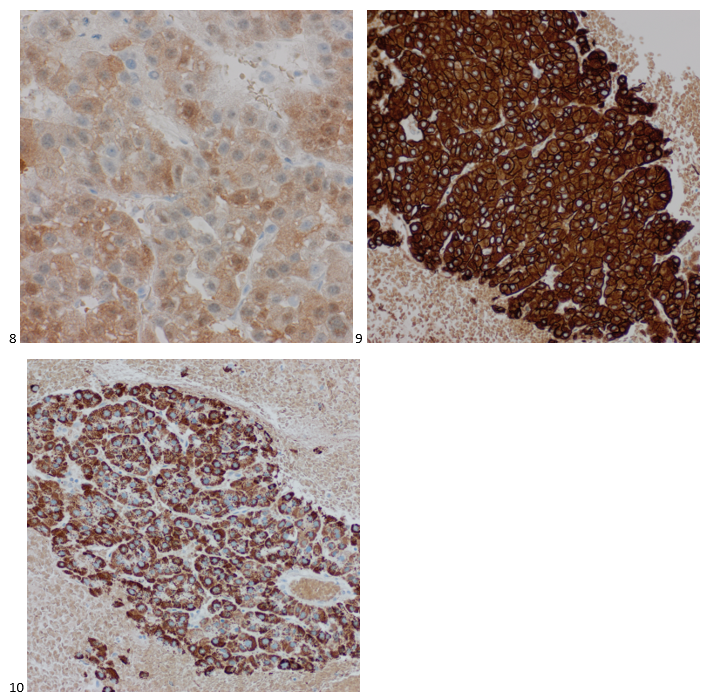
Immunostains were performed using proper positive and negative controls on the cell block sections, and the tumor cells show positive staining for Arginase, cam5.2, and Hepar1, while negative staining for CK7 and PAX8 (not shown).
Fortunately, before ordering immunostains, both our cytologist and pathologist working on the case peered into the patient’s medical record and noticed that he had recent bloodwork which demonstrated a positive Hepatitis C screening. This diagnosis was as recent as the identification of his humerus mass. Had it not been for his car accident, I can’t imagine how long he would have gone undiagnosed for both hepatitis and metastatic hepatocellular carcinoma. Incidental findings save lives, folks.
Granted, in settings of unknown primaries with widespread metastatic disease, such as carcinomatosis, an extensive workup is almost always inevitable. Narrowing down possible etiology based on information such as gender, age, and environmental or occupational exposure can help, but that doesn’t always yield a definitive answer as time- or cost-effectively as possible. In this case, that one clue of untreated Hepatitis C was all the cytopathology team needed. A rarity, sure, but as we are asked to do more personalized tests with less material, think of the patient’s specimen as a puzzle and keep your eye out for a clue both under the microscope and behind the computer. You never know what you might find that reduces errors and unnecessary testing while efficiently leading to a definitive diagnosis.

-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.