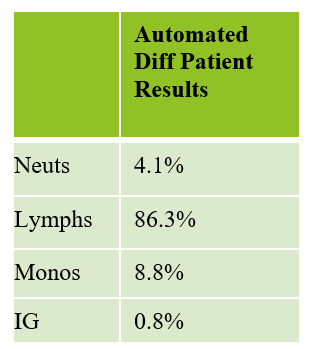
A healthy 30 year old woman visited her primary care physician concerned about a rash with questionable infection on her hands. The physician prescribed an antibiotic for infection and ordered a CBC. From the results below, it can be seen that the patient had a pancytopenia and a relative lymphocytosis.

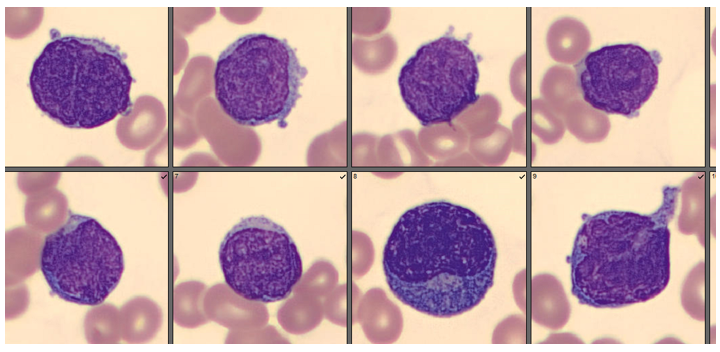
A manual differential was performed on CellaVision and the presence of large, clefted lymphocytes with immature features was noted. A request for pathology review was sent to the pathologist. The pathologist’s review stated “ Atypical lymphocytosis, specimen to be submitted for flow cytometry. Report to follow. Occasional atypical lymphocytes with immature features also noted. Lymphocyte population is predominantly mature”
The peripheral blood sample was sent out for immunophenotyping by flow cytometry and FISH studies. Flow cytology reported “precursor B-cell population expressing CD19, CD10, HLA-DR, and CD34 is identified. Percent of abnormal cells, 30%. These findings are consistent with precursor B-lymphoblastic leukemia.” While we tend to associate a leukemia diagnosis with a high white blood cell count, and the presence of blasts, this patient was unusual in that she did not have a high WBC or blasts seen on the peripheral smear. Pancytopenia in ALL has been noted in literature. A study of new onset pancytopenia in adults showed that the majority of cases were acute myeloid leukemia, but ALL and other lymphomas also caused pancytopenia3. Another study noted that “pancytopenia followed by a period of spontaneous recovery may precede the diagnosis of acute lymphoblastic leukemia.”1 While the pathologist did not identify blasts on this differential, and cells were predominately mature, WBC was very low, and our analyzer did flag “?blasts/abnormal lymphs” and reflexed the manual differential.

Leukemia is a broad term that includes a number of different chronic and acute diagnoses. Chronic and acute forms are further broken down into myeloid and lymphoid and then into subtypes. The French-American-British (FAB) classification of acute leukemias was devised in the 1970’s and 1980’s and was based on cytochemical staining and morphology of cells. These tests were performed manually and relied on what the cells look like under the microscope. The series of stains were used to differentiate myeloblasts from lymphoblasts. I’m old enough that I remember learning about these stains when they were being developed and thinking how amazing they were!
We’ve come a long way since the early 1980’s! Although the FAB diagnostic criteria are not entirely forgotten, the World Health Association (WHO) classification, first published in 2001, has largely replaced the FAB classification. The newest guidelines for Acute Lymphoblastic Leukemias (ALL) were published by WHO in 2016. These new guidelines supplement morphology and cytochemical staining with newer testing which can now identify and distinguish B cell and T cell ALL. In making a diagnosis, peripheral blood and/or bone marrow aspirate samples are subject to flow cytometry immunophenotyping and chromosome testing such as cytogenics or fluorescence in situ hybridization(FISH). Molecular tests can also be done to look for specific gene changes in the leukemia cells. The WHO classification has become preferred because these new tests can give more information that is important for treatment. Prognosis for ALL depends on patient age, WBC counts at diagnosis and these specific test results which tell us which subtype of ALL is present. The presence and identification of chromosomal alterations is important for diagnosis and therapy decisions. Identifying chromosomal alterations can also lead to better risk classification which is significant because of the knowledge that, while rearrangements tend to have poorer outcomes, some rearrangements actually offer a better prognosis. With the future era of individualized, targeted therapy for leukemia, combining conventional cytogenics with molecular and FISH methods will greatly enhance the accuracy of information and provide patients with more specific and customized treatment options.
While ALL is the most common childhood leukemia, it is not as commonly seen in adults. B cell ALL is more common than T cell ALL in all ages, and accounts for about 90% of ALL cases in children and about 75% of ALL cases in adults. Cure rates in children exceed 90% but in adults varies with age and depending on chromosomal alterations. Most B cell ALL subtypes with chromosome translocations tend to have a poorer outcome than those without translocations. As well, younger adults, <50 years old, have better prognosis than older adults.
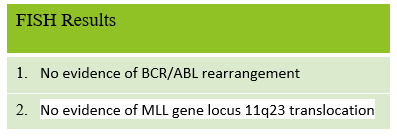
This patient did not have a BCR/ABL rearrangement or MLL gene locus 11q23 translocation, which both carry poorer prognoses, but she also did not have a translocation between chromosome 12 and 21 or more than 50 chromosomes, both of which offer more favorable prognoses. This young woman therefore would be in an average risk category and appears to have been diagnosed very early in the course of her disease. We have not seen any further workup, as the patient is being treated at another facility. We wish her well in her leukemia treatments.
References
- Hasle H, Heim S, Schroeder H, et al. Transient pancytopenia preceding acute lymphoblastic leukemia (pre-ALL). Leukemia. 1995 Apr;9(4):605-608.
- Iacobucci I, Mullighan CG. Genetic Basis of Acute Lymphoblastic Leukemia. J Clin Oncol. 2017 Mar 20;35(9):975-983. doi: 10.1200/JCO.2016.70.7836. Epub 2017 Feb 13. PMID: 28297628; PMCID: PMC5455679
- Bone Marrow evaluation in new onset pancytopenia. Human Pathology. Vol 44, Issue 6. June 2013
- Hematology: Basic Principles and Practice, 7th Edition. Ronald Hoffman, Edward J. Benz, et al. 2018 Elsevier

-Becky Socha, MS, MLS(ASCP)CMBBCM graduated from Merrimack College in N. Andover, Massachusetts with a BS in Medical Technology and completed her MS in Clinical Laboratory Sciences at the University of Massachusetts, Lowell. She has worked as a Medical Technologist for over 40 years and has taught as an adjunct faculty member at Merrimack College, UMass Lowell and Stevenson University for over 20 years. She has worked in all areas of the clinical laboratory, but has a special interest in Hematology and Blood Banking. She currently works at Mercy Medical Center in Baltimore, Md. When she’s not busy being a mad scientist, she can be found outside riding her bicycle.
