Case History
A 20 year old female with no significant past medical history presented with a painful pruritic rash on the bilateral inner thighs that had been persistent for one month. Prior to presentation, she had been treated with oral and topical antihistamines, topical steroids, valacyclovir, and partial courses of doxycycline and cephalexin without improvement. Physical examination was notable for diffuse erythema and dermal edema of the bilateral medial thighs with superimposed exophytic papules with dark, necrotic cores, the largest of which measured 1 cm in diameter (Image 1). Punch biopsy of the lesions was taken and sent for histology. A sample from necrotic tissue was sent to microbiology laboratory for gram stain and cultures.
Laboratory diagnosis
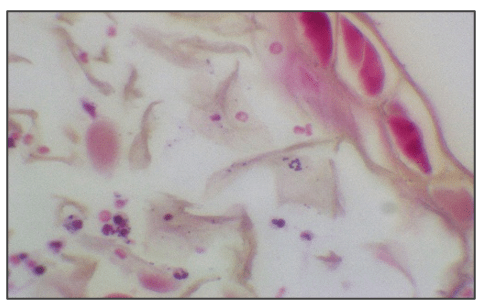
Gram stain showed gram positive cocci in clusters. After 32 hours of incubation, tissue cultures grew white, β-hemolytic colonies which were catalase positive, coagulase negative, and pyrrolidonylarylamidase (PYR) positive. The organism was identified as Staphylococcus lugdunensis by MALDI-TOFmass spectrometry. Histology revealed eosinophilic inclusions consistent with molluscum bodies as well as inflammatory infiltrate (Image 2). Brown and Hopps stain on tissue showed Gram-positive cocci is small clusters (Image 3). A diagnosis of molluscum contagiosum superinfected with Staphylococcus lugdunensis was made based on laboratory and histologic findings.


Discussion
S. lugdunensis is a coagulase-negative staphylococcus first isolated in 1988 that was initially thought to be a commensal skin organism but has been shown to cause skin and soft tissue infections (SSTIs), bacteremia, endocarditis, prosthetic joint infections, and osteomyelitis,2 with a virulence more similar to S. aureus than to that of other coagulase-negative staphylococci. SSTIs are one of the more common manifestations of S. lugdunensis infection; one analysis of 229 S. lugdunensis clinical isolates demonstrated that 55.4% were associated with SSTIs.3 The spectrum of S. lugdunensis-related SSTIs includes folliculitis, pustulosis, cellulitis, abscesses, and rarer secondary infection of molluscum contagiosum and hidradenitis suppurativa.5 Molluscum superinfection itself is a rare phenomenon, and when it occurs, the superinfecting agent is most often S. aureus.1 Our case suggests that S. lugdunensis should also be considered as a potential causative agent of molluscum superinfection. There is growing recognition that S. lugdunensis is a virulent pathogen that should not be disregarded as a contaminant if found on culture. Importantly, when compared with S. aureus, S. lugdunensis has a more limited resistance profile; methicillin resistance is still uncommon, and 74.6% of isolates in one recent study were penicillin susceptible.4 Awareness of this more favorable resistance profile can facilitate selection of narrower-spectrum antibiotic therapies for S. lugdunensis infections.
In our case, patient received one dose of vancomycin and metronidazole in the emergency department and was then started on cefazolin for cellulitis. After wound culture identified S. lugdunensis, the patient was discharged on cefadroxil 1g twice daily for 10 days. On follow up, the rash had resolved.
References
- Berger EM, Orlow SJ, Patel RR, Schaffer JV. Experience With Molluscum Contagiosum and Associated Inflammatory Reactions in a Pediatric Dermatology Practice: The Bump That Rashes. Arch Dermatol. 2012;148(11):1257–1264. doi:10.1001/archdermatol.2012.2414
- Douiri N, Hansmann Y, Lefebvre N, Riegel P, Martin M, Baldeyrou M, Christmann D, Prevost G, Argemi X. Staphylococcus lugdunensis: a virulent pathogen causing bone and joint infections. Clinical Microbiology and Infection, 2016;22(8):747-748. doi:10.1016/j.cmi.2016.05.031
- Herchline TE, Ayers LW. Occurrence of Staphylococcus lugdunensis in consecutive clinical cultures and relationship of isolation to infection. J Clin Microbiol. 1991;29(3):419–421.
- Taha L, Stegger M, Söderquist B. Staphylococcus lugdunensis: antimicrobial susceptibility and optimal treatment options. Eur J Clin Microbiol Infect Dis. 2019;38(8):1449–1455. doi:10.1007/s10096-019-03571-6
- Zaaroura H, Geffen Y, Bergman R, Avitan‐Hersh E. Clinical and microbiological properties of Staphylococcus lugdunensis skin infections. J Dermatol, 2018;45: 994-999. doi:10.1111/1346-8138.14496

-Ansa Mehreen, MD. 1st year AP/CP resident at University of Chicago hospital program based at Evanston Hospital. Her academic interests include gastrointestinal pathology.

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois. Follow Dr. McElvania on twitter @E-McElvania.
