Case History
A 24 year old male with a past medical history of recurrent streptococcal pharyngitis presents to the emergency department with a sore throat and dyspnea. His symptoms began three days prior and included left-sided upper neck and lower jaw pain and odynophagia. The patient’s evaluation demonstrated tachycardia, cervical lymphadenopathy, and a small left tonsillar abscess. Labs were significant for an elevated WBC count but blood cultures, Group A streptococcal and mononucleosis screens were negative. The patient was admitted for pain management and treated with a combination of IV ampicillin/sulbactam (amp/sulb) and steroids. He improved with treatment and was discharged the following day on oral amoxicillin/clavulanic acid (amox/clav). Nine days later, the patient re-presented with similar complaints. The tonsillar abscess had increased in size to 2cm. Labs were significant for leukocytosis and a now positive Group A streptococcal screen. 2mL of pus was aspirated from the lesion but no cultures were ordered. The patient’s status again improved, and he was discharged home again on oral amox/clav. The patient returned the following day and was placed on IV amp/sulb and admitted for imaging and symptom management. A neck CT with contrast revealed a now 3cm tonsillar abscess with reactive cervical lymphadenopathy (Image 1). A throat culture was collected; however, no beta-hemolytic streptococci were recovered after 48 hours of incubation. Incision and drainage of the abscess was performed at bedside, recovering an additional 10 mL of purulence that was sent to the microbiology laboratory for aerobic and anaerobic culture. The patient improved on IV amp/sulb and was switched to high dose amox/clav on day 15.
Laboratory Identification
Gram stain of the aspirated purulence revealed many WBCs and a mixture of gram positive rods and cocci (Image 2). The aerobic culture grew a heavy amount of tiny, weakly beta-hemolytic colonies on blood agar. Smears of these colonies revealed Gram-positive coryneform rods. Biochemical testing determined the growth to be catalase-negative and MALDI-TOF MS definitively identified the organism as Arcanobacterium haemolyticum. The anaerobic culture grew oral flora.



Discussion
A. haemolyticum is an infrequently isolated gram positive rod which is an etiologic agent of non-streptococcal pharyngitis diagnosed predominantly in adolescents or young adults. The diagnosis of A. haemolyticum can be challenging because itis often clinically indistinguishable from cases caused by beta-hemolytic streptococci. Most patients exhibit some degree of cervical lymphadenopathy, and a scarlatiniform rash can be present in up to 50% of cases. From a laboratory perspective, A. haemolyticum is slowly growing and weakly beta hemolytic after 24-48 hours on media containing sheep blood (including SBA and Strep Selective agars routinely used for screening throat cultures). The beta-hemolytic activity of A. haemoltyicum is attributed to expression of arcanolysin, a cholesterol-dependent cytolysin. Interestingly, arcanolysin more robustly binds to rabbit and human erythrocytes than those from sheep,1 which may explain the organism’s weak beta hemolysis on routine media. In this setting, the organism can be missed or dismissed as commensal flora without careful observation. Conversely, if beta-hemolysis is observed, the colony morphology and catalase non-reactivity can lead to misidentification as beta-hemolytic streptococci in the absence of a Gram stain or other determinative methods (i.e. MALDI-TOF MS).
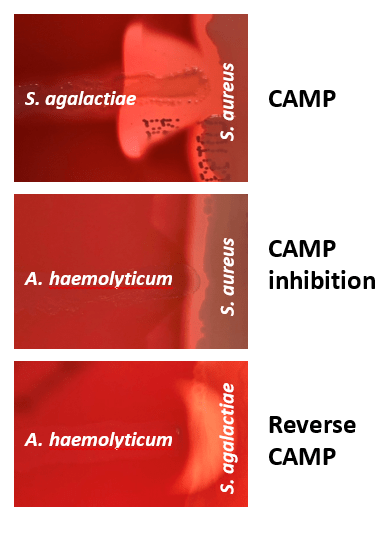
The beta hemolysis of this patient’s A. haemolyticum isolate is difficult to appreciate in reflected (room) light, and was best observed after 48 hours using transduced light from a light box (Image 3). A. haemolyticum displays CAMP inhibition due to the production of phospholipase D which inhibits the hemolytic activity of beta-lysin produced by S. aureus (Image 4) and is reverse-CAMP positive when perpendicular to Group B streptococci which can aid in identification.2
Erythromycin is the drug of choice for treatment of A. haemolyticum, further highlighting the need for definitive identification of this organism in settings of pharyngitis. The use of penicillin for treatment of A. haemolyticum pharyngitis can result in treatment failure, possibly due to invasion of host cells, thus establishing a reservoir,3 or due to a penicillin-tolerant phenotype.4 It is unclear in this case if source control or decreased susceptibility necessitated the multiple courses of antibiotics utilized. Fortunately, the patient’s symptoms resolved on high dose amoxicillin/clavulanic acid following thorough incision and drainage. He subsequently returned for an outpatient tonsillectomy.
References
- Jost BH, Lucas EA, Billington SJ, Ratner AJ, McGee DJ. 2011. Arcanolysin is a cholesterol-dependent cytolysin of the human pathogen Arcanobacterium haemolyticum. BMC Microbiology 11:239.
- Kang H, Park G, Kim H, Chang K. 2016. Haemolytic differential identification of Arcanobacterium haemolyticum isolated from a patient with diabetic foot ulcers. JMM Case Reports.
- Österlund A. 1995. Are Penicillin Treatment Failures in Arcanobacterium haemolyticum Pharyngotonsillitis Caused by Intracellularly Residing Bacteria? Scandinavian Journal of Infectious Diseases 27:131-134.
- Nyman M, Danek G, Thore M. 1990. Penicillin Tolerance in Arcanobacterium haemolyticum. The Journal of Infectious Diseases 161:261-265.
-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern in the Department of Pathology and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.
