Since I last wrote about some testing options available for COVID-19 testing just 1 month ago, many things have changed in the regulatory requirements, and the companies offering testing options. With that in mind along with the fact that things will likely continue to changes, I’ll write to address current and future challenges facing COVID-19 laboratory testing.
- What control material can be used?
- How can I make specimens safe?
- Supply chain issues and solutions.
- False Negative results of COVID-19 tests: what to tell clinicians.
- Serology Tests: Future Testing and Challenges
Control Material
As the FDA said contrived specimens could be used, that means that RNA can be spiked into a clinical matrix for extraction. While this began with a requirement for genomic RNA, it has been loosened to include plasmid DNA. However, I would caution against using plasmid DNA, because when it is amplified, it can easily cause contamination and unlike RNA, DNA can persist in the environment for a long time. I once hear a story about a lab director who thought they were very careful, but in pipetting, they contaminated the lab in 3 days and it had to be cleaned up for 4 weeks.
We had some issues using in vitro transcribed RNA (of just the N-gene) and genomic RNA, because the recovery was very low. We found out that intact viral particles were better in optimization experiments using control endemic SARS strains (Zeptometrix controls, Table 1). The free RNA Ct values fell sharply (over 1000-fold) when added to Nasopharyngeal (NP) matrix or Viral Transport Media (VTM). However, much lower levels of the encapsulated viral control had consistent levels of amplification.
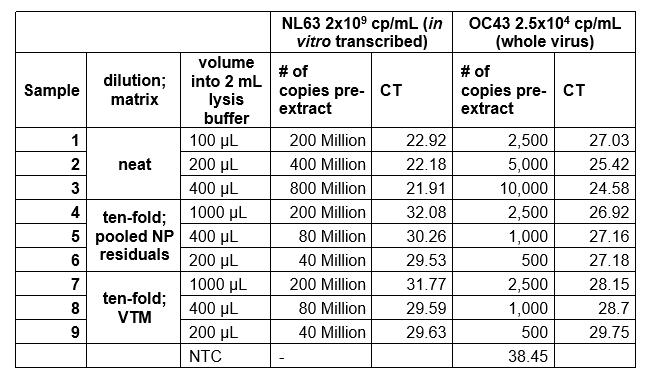
Table 1. Amplification of free viral RNA vs. viral particles when added to matrix
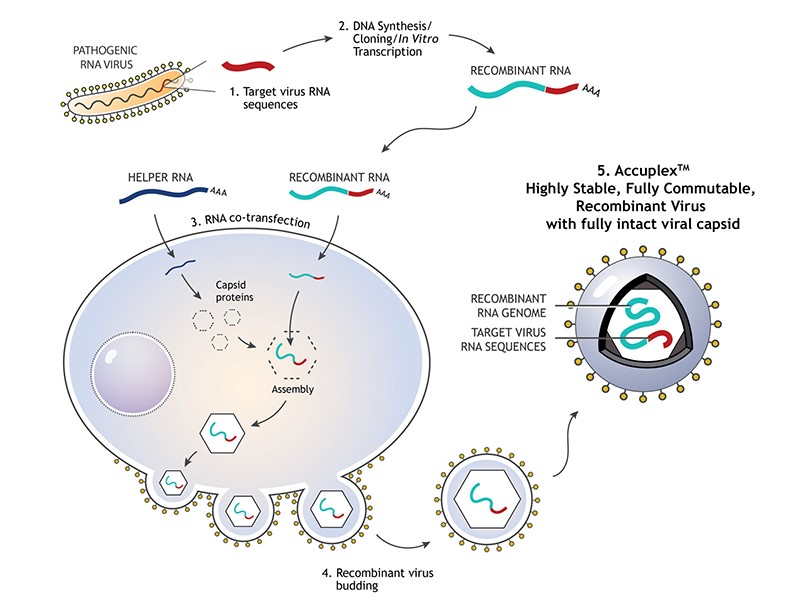
Therefore, we used a synthetically encapsulated SARS-CoV-2 RNA sample called Accuplex (SeraCare, Figure 1), which gave good recovery and a limit of detection down to 260 copies/ mL (5 copies/ reaction). Alternative similar material that we have not evaluated include: COVID-19 RNA synthesized inside inactivated E coli (Zeptometrix) and Armored RNA (Asuragen).
Lab Safety of Specimens
A safety recommendation of the FDA was to perform extraction of samples in a Biosafety level 2 hood. However, high-throughput extraction can’t be easily done this way. For us, we had to prepare samples in the hood then take them to the stand-alone closed system extractor. Our Micro fellow had the creative idea to do “Off-Board” lysis, which would inactivate the virus in the hood before walking it over. We later found that combining lysis with NP matrix before spiking RNA stabilized the RNA for accurate measurement. We were able to find an LOD of 14 copies/ reaction this way.
Some labs have proposed using heat inactivation (~30 minutes at 50-60C) of virus as a safety measure, but the published literature available on how that affects sensitivity is lacking currently.
Supply Chain issues
You have surely heard about all of the new companies that have come out with new testing platforms and assays for COVID-19 testing by now. However, the downside is that unless you already have their instrument, you likely won’t be able to get reagents in time to perform the assay. Even if you do have an instrument, limited resources are necessitating allocation based on high risk areas, so you are likely to receive fewer kits than you would like. Also, the reference labs are still ramping up capacity and are returning results back with long turnaround times currently (~ 1 week). This supports the strategy to bring the testing in-house, so that you can get results back quickly and have control over at least your labs reagent supply. If you have the instrumentation of another FDA approved EUA, you can start performing testing if you follow that protocol exactly- the CDC is the most widely used.
False Negative Tests of COVID-19
This is hard to assess when only one lab testing modality (PCR) is available, but clinicians report negative results in a patient with classic symptoms and a contact history with a COVID-19+ person. Given the impressive analytic sensitivity of the test (generally 1 copy of RNA in 1mL of sample), the likely explanation is that there is a specimen issue. Proper NP sampling requires sticking the swab to the very back of the nasal cavity. Furthermore, this virus may reside more in the lower respiratory track (lungs) and simply not be present in the area sampled. This is why repeat sampling could be helpful. However, the outcome should be the same whether or not you have a negative test: if you have symptoms you should self-isolate unless you require emergent care due to shortness of breath or other symptoms that can’t be managed at home. The lab is familiar with these pre-analytic limitations that can arise, but it is helpful to explain this to clinicians.
Serology Tests: Future Testing and Challenges
Serology can be very helpful as a separate method from qPCR to determine if someone has been infected with SARS-CoV-2. Notice, that is in the past tense. A small (n=9) pre-print study from Nature indicates serologic conversion starts around day 8 or 10 after symptom onset, which often is not in a clinically helpful timeframe. However, these tests are cheaper and easier to perform, so could be useful for epidemiological purposes to determine who has been infected with COVID-19. Early genetic data indicates that the mutation rate is slow (4x slower mutation rate compared to seasonal flu) as one would suspect for RNA-based viruses, so the virus shouldn’t change enough to cause re-infection in someone with sufficient antibody levels.

However, several challenges in interpreting these antibody tests include:
- Some conflicting data as to how quickly IgM develops relative to the onset of symptoms
- What is the time-line for IgG production?
- Ruling out cross reactivity with other strains of Coronavirus that cause upper respiratory infections.
References
- Wolfel R, Corman VM, Guggemos W et al. Virological assessment of hospitalized patients with COVID-2019. Nature epub ahead of print. https://www.nature.com/articles/s41586-020-2196-x_reference.pdf
- Mitchell S, George K et al. Verification procedure for commercial tests with Emergency Use Authorization for the detection of SARS-CoV-2 RNA. American Society of Microbiology
- https://www.livescience.com/coronavirus-mutation-rate.html

-Jeff SoRelle, MD is a Chief Resident of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and improving genetic variant interpretation.
