Case History
43 year old man presented with symptoms of superior vena cava syndrome including swelling of the head and neck and difficulty breathing. He was found to have a 9 cm anterior mediastinal mass on imaging.
Excisional Biopsy

Bottom: Small lymphocytes with scattered large multinucleated Hodgkin and Reed-Sternberg (HRS) cells.
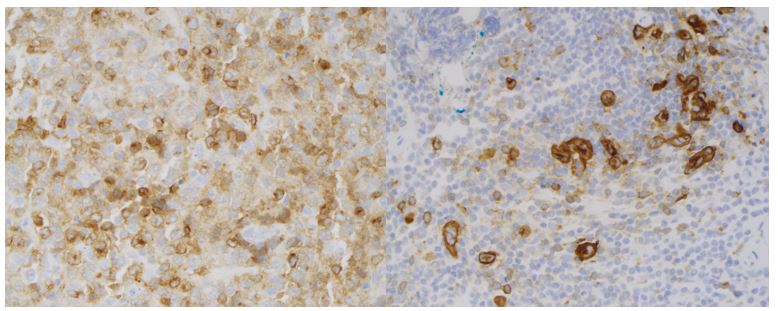
Right: CD30 highlighting Hodgkin and Reed-Sternberg cells with a golgi and membranous staining pattern.
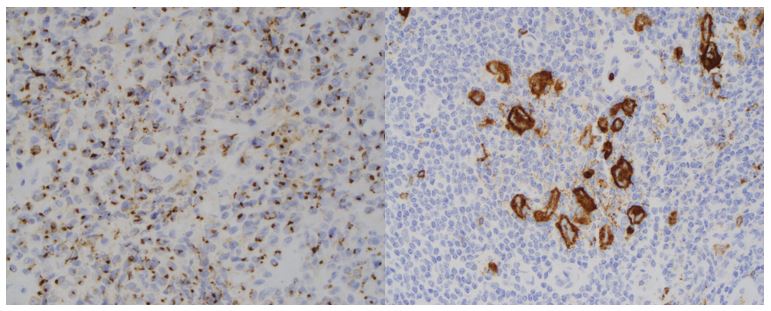
Right: CD15 highlighting Hodgkin and Reed-Sternberg cells with a golgi and membranous staining pattern.
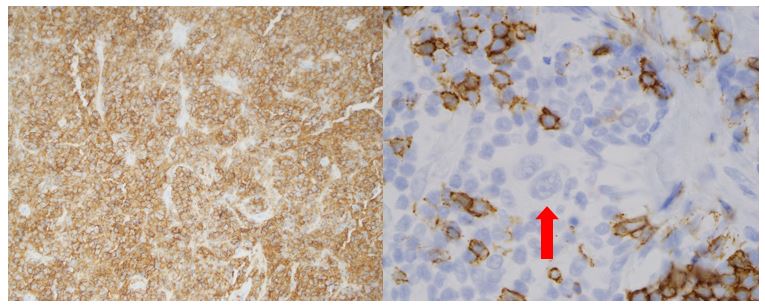
Right: CD20 highlighting small B-cells surrounding a negative HRS cell.
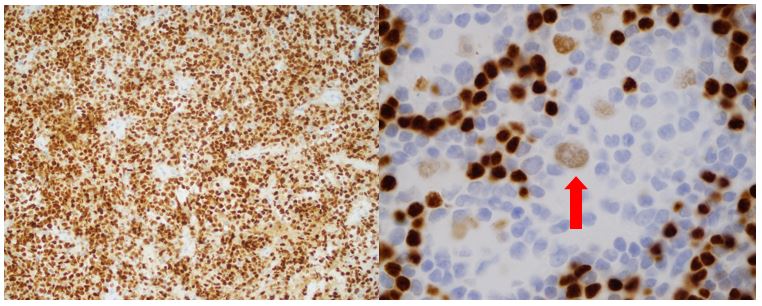
Right: PAX5 showing bright staining in small B-cells surrounding a dimly stained HRS cell.

Right: Ki-67 showing increased staining in the HRS cells.
Diagnosis
Sections show fragments of fibrotic tissue with crush artifact. Two distinct morphologies are seen in different tissue fragments. Some tissue fragments show infiltration by cords and aggregates of abnormal large lymphoid cells with irregular nuclear contours, somewhat vesicular chromatin, small nucleoli and small to medium amounts of cytoplasm. Frequent apoptotic cells and mitotic figures are seen. In other tissue fragments, the large cell component is absent and there are focally vague nodules. The nodules are composed of small mature appearing lymphocytes, rare eosinophils and scattered medium and large mononuclear and multinucleated cells with prominent nucleoli consistent with Hodgkin cells and Reed-Sternberg cells, respectively. Admixed histiocytes are also seen.
By immunohistochemistry, the areas with different morphologies also show different staining patterns. The areas with the large cell infiltrate are immunoreactive for CD20, BCL6, and MUM1, dimly positive or negative for CD45 and negative for CD10. CD30 is variably positive in the large cell population and CD23 is largely negative. CD15 shows a golgi staining pattern. The Hodgkin and Reed-Sternberg (HRS) cells present in the areas without the large cell infiltrate are brightly immunoreactive for CD30 and CD15 (membranous and golgi pattern), dim positive for PAX5 and are negative for CD20. CD20 and PAX5 highlight small B-cells present in aggregates surrounding the HRS cells. By Ki-67 staining, the proliferation index is high (90%) within the diffuse large cell component and also highlights the HRS component.
Overall, the findings are of a composite lymphoma composed of both a diffuse large B-cell lymphoma (DLBCL) and a classic Hodgkin lymphoma (CHL).
Discussion
Composite lymphomas occur when two morphologically and immunophenotypically distinct lymphomas occur at the same anatomical site. They are most commonly composed of two Non-Hodgkin B-cell lymphomas (NHL), however rare cases of composite CHL with NHL have been reported. In a review of the literature, Goyal et. al. documented 20 previously reported cases of composite lymphoma with CHL and DLBCL components. The median age at presentation was 51 years with 12 men and 9 women. Fifteen of the cases presented with nodal involvement and of those, three had mediastinal disease. The most common subtype of CHL was nodular sclerosis. Evaluation for IGH gene rearrangements was performed on both components of 6 cases, with either a complete or partial clonal relationship between the components seen in all of the cases tested. This suggests a shared origin from a common B-cell precursor.1
A review of literature by Wang et. al. documented 10 previously described composite lymphomas consisting of DLBCL and CHL. The most common site of occurrence was in lymph nodes, followed by three cases seen in the stomach, one case in the small intestine and one case in the anterior mediastinum. CHL is more commonly associated with EBV infection than NHL In the reviewed cases, 6 showed positivity for EBV infection in both the DLBCL and CHL components. This suggests that the lymphomas shared a common EBV-infected progenitor cell, and are also clonally related as seen in the Goyal review. 2
Composite lymphomas must be distinguished from another WHO defined entity called B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classic Hodgkin lymphoma. This entity has previously been referred to as “grey-zone lymphoma.” These lymphomas tend to present as mediastinal masses and can cause superior vena cava syndrome. They show a wide spectrum of histologic appearances within a single tumor and often show sheet-like growth of pleomorphic cells. Some areas may resemble CHL while others resemble DLBCL. The neoplastic cells typically do not show the characteristic immunophenotype of either CHL or DLBCL. Areas that may resemble CHL will show preservation of B-cell markers, while areas more characteristic of DLBCL might lose B-cell markers and express CD30 and CD15. These tumors will show clonal rearrangement of the immunoglobulin genes. They tend to have a more aggressive clinical course and worse outcome than either CHL or DLBCL. 3
This case was ultimately diagnosed as a composite lymphoma (CL) because it consisted of separate areas with the morphologic and immunophenotypic features of both classic Hodgkin lymphoma and diffuse large B-cell lymphoma. Patients tend to have a poor prognosis with short survival. There is no standardized treatment for composite lymphomas due to their rare occurrence; however cases with a component of DLBCL are generally treated with aggressive chemotherapy such as R-CHOP.
References
- Goyal, G. et al. “Composite Lymphoma with Diffuse Large B-Cell Lymphoma and Classical Hodgkin Lymphoma Components: A Case Report and Review of the Literature.” Pathology – Research and Practice vol. 212,12(2016):1179-1190. http://www.ncbi.nlm.nih.gov/pubmed/27887763.
- Wang, Hong-Wei et al. “Composite diffuse large B-cell lymphoma and classical Hodgkin’s lymphoma of the stomach: case report and literature review” World journal of gastroenterology vol. 19,37(2013):6304-9.
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoetic and Lymphoid Tissues (Revised 4th edition). IARC: Lyon 2017.

–Chelsea Marcus, MD is a Hematopathology Fellow at Beth Israel Deaconess Medical Center in Boston, MA. She has a particular interest in High-grade B-Cell lymphomas and the genetic alterations of these lymphomas.
