Case History
53 year old female was found to have leukocytosis upon a wellness examination. A CBC was performed and found a WBC of 34.0, HgB 13.2, and Plt of 263,000. The WBC differential consisted of 80% Lymphocytes and 12% neutrophils. The patient states that she is feeling well, no fever, chills, or night sweats. She denies any adenopathy. Flow Cytometry was recommended as well as morphologic review along with Cytogenetics and FISH (fluorescence in-situ hybridization).
Lab Identification
CBC
| WBC 33.68 [103/uL] | NEUT 4.17 [103/uL] 12.3 [%] |
| RBC 4.54 [106/uL] | LYMPH 26.91 [103/uL] 79.9 [%] |
| HGB 13.2 [g/dL] | MONO 2.04 [103/uL] 6.1 [%] |
| HCT 40.0 [%] | EO 0.39 [103/uL] 1.2 [%] |
| MCV 88.1 [fL] | BASO 0.11 [103/uL] 0.2 [%] |
| MCH 29.1 [pg] | IG 0.06 [103/uL] 0.2 [%] |
| MCHC 33.0 [g/dL] | NRBC 0.00 [103/uL] 0.0 [%] |
| RDW-CV 14.3 [%] | |
| PLT 263 [103/uL] | |
| MPV 9.4 [fL] |
Morphologic Review


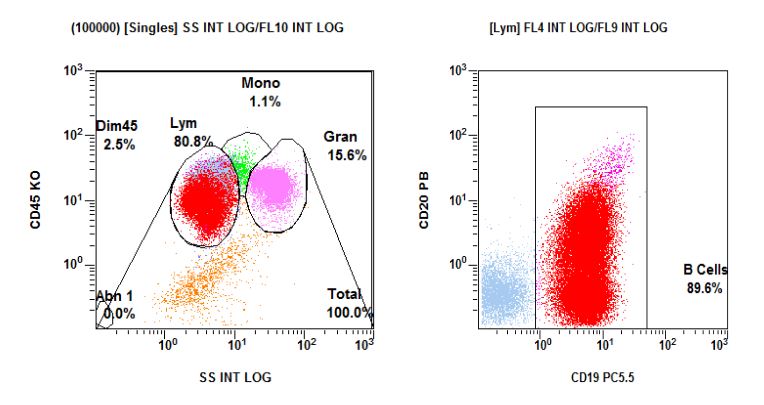
Flow Cytometry: Population of Interest – Abnormal Lymphocytes
Cytogenetics: 46,XX[20] Normal Female Karyotype
It is not unusual to observe a normal karyotype in CLL due to the limited number of abnormal cells and/or low spontaneous proliferative activity of the malignant cells. Fluorescence in situ hybridization studies may identify cytogenetic abnormalities of prognostic significance in interphase nuclei not observed in the metaphase cells analyzed. In cases of CLL molecular profiling may be performed to aid in predicting course of the disease. If clinically indicated these studies may be considered. Standard cytogenetic analysis may not detect subtle submicroscopic rearrangements and may not include metaphases from abnormal cell populations with low mitotic rates or present in low levels.
| Metaphases Counted: 20 | Metaphases Analyzed: 20 |
| Metaphases Karyotyped: 2 | Culture Type: 48EB, 72IL2/DSP30 |
| Banding Technique: GTG | Banding Resolution: 400 |
Fluorescence in-situ Hybridization: Abnormal – 13q14 deletion present
Fluorescence in situ hybridization (FISH) analysis was performed using a specific set of probes for Chronic Lymphocytic Leukemia (CLL). This study revealed a 13q14 deletion. Counts for all other probes were within the normal reference range. This finding represents an ABNORMAL result. Deletion of 13q14 is the most common deletion in CLL being reported in 10-20% of cases by conventional cytogenetics and up to 64% of cases by FISH analysis. When present as a sole abnormality this deletion is associated with a good prognosis and a median survival longer than CLL patients with a normal karyotype.
| Del(6q) | Not Detected |
| Del(11q)(ATM) | Not Detected |
| Trisomy 12 | Not Detected |
| Del(13q)/-13 | DETECTED |
| t(11;14) | Not Detected |
| Del(17p)(TP53) | Not Detected |
Discussion
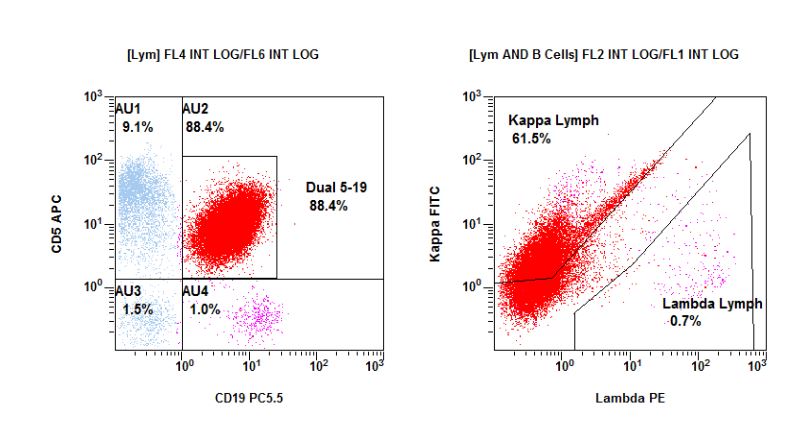
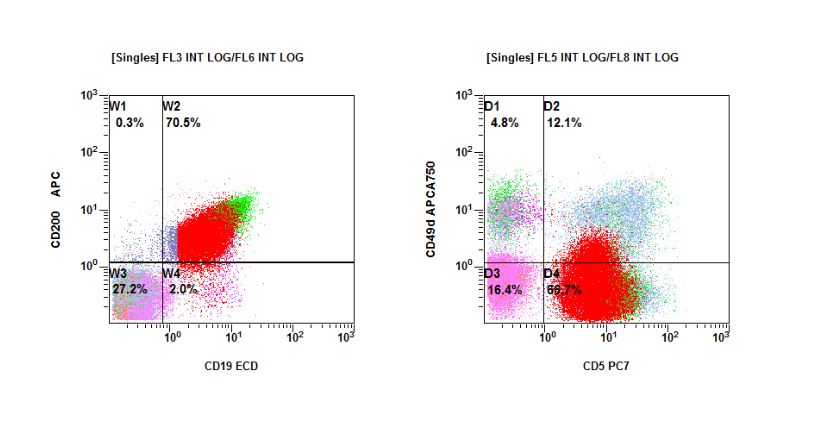
Chronic Lymphocytic Leukemia is a neoplasm of about 5 cases per 100,000 people with a median age of around 70 years old. The neoplasm is composed of monotypic mature B-cells that typical express CD5. Other immunophenotypic characteristics of the leukemic B-cells include CD19, CD20, CD22, and CD79b with dim surface expression of one of the immunoglobulin light chains, Kappa or Lambda. These cells typically express CD200 which helps differentiate the leukemia from Mantle Cell Lymphoma/Leukemia. Patients found to have a mutated IGHV genes typically have a better prognosis than those with an unmutated genes. Expression of ZAP70, CD38, or CD49d is also associated with an adverse prognosis. Complex karyotypes also trend towards a poor outcome. Adverse predictive factors include rapid lymphocyte proliferations in the blood, typically doubling in < 12 months.
Monoclonal B-cell Lymphocytosis is typically characterized as a monoclonal
BCell count of <5 X109/L in the peripheral blood. Monoclonal B-cell Lymphocytosis with a Chronic Lymphocytic Leukemia-type phenotype is the most common which accounts for about 75% of all cases. It has been reported that virtually all Chronic Lymphocytic Leukemias are preceded by Monoclonal B-cell Lymphocytosis, although not all MBLs progress to CLL.
References
- Dohner H, et al. N Engl J Med 2000; 343:1910-6.
- Hamblin TJ.Best Practice & Research Clinical Haematology. 2007; 20(3):455 – 68.
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H. WHO classification of tumours of haematopoietic and lymphoid tissues, fourth edition. Lyon, France: IARC; 2017
- Nowakowski GS, et al. Br J Hematol. 2005; 130:36 – 42.
- Atlas of Genetics and Cytogenetics in Oncology and Hematology http://atlasgeneticsoncology.org/

Troy G. Krieger, MS, MLS(ASCP)CMSCYMCMQLSCMCLS(MT) graduated from Montana State University Billings with a BS in Biology, Medical Laboratory Science option. He received a NAACLS Certificate and clinical training from the University of North Dakota in Grand Forks, ND, where he also received his Master’s degree. He is a Medical Laboratory Scientist / Flow Cytometrist at Yellowstone Pathology Institute, Inc in Billings, MT and his interests include Hematology, Immunopathology, and Flow Cytometry.
