Case History
A 45 year old male underwent a chest MRA for aortic dilation due to his history of an aneurysmal aortic root. Upon imaging, an incidental anterior mediastinal mass was seen that measured 4.0 cm. In preparation for an upcoming cardiac surgery, the patient underwent a thymectomy with resection of the mass. The sample is a section from the mediastinal mass.
Diagnosis

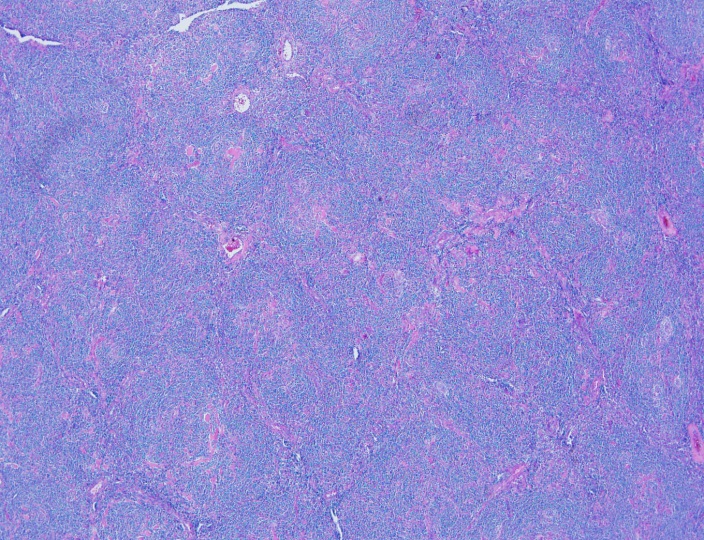

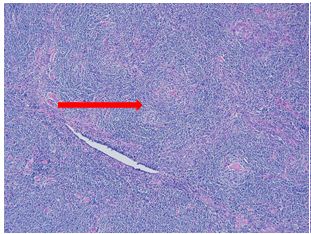
Sections show an enlarged lymph node with several follicles demonstrating atrophic-appearing germinal centers which are primarily composed of follicular dendritic cells. These areas are surrounded by expanded concentrically arranged mantle zones. Focal “twinning” of germinal centers is present. Additionally, prominent centrally placed hyalinized vessels are seen within the atrophic germinal centers giving rise to the “lollipop” appearance.
By immunohistochemistry, CD20 highlights B-cell rich follicles while CD3 and CD5 highlight abundant T-cells in the paracortical areas. CD10 is positive in the germinal centers while BCL2 is negative. CD21 highlights expanded follicular dendritic meshwork. CD138 is positive in a small population of plasma cells and are polytypic by kappa and lambda immunostaining. HHV8 is negative. MIB1 proliferation index is low while appropriately high in the reactive germinal centers.
Overall, taking the histologic and immunophenotypic findings together, the findings are in keeping with Castleman’s disease, hyaline vascular type. The reported clinical and radiographic reports suggest a unicentric variant.
Discussion
Castleman’s disease comes primarily in two varieties: localized or multicentric. The localized type is often classified as the hyaline vascular type (HVCD). Demographically, it’s a disease of young adults but can be found in many ages. The most common sites for involvement are the mediastinal and cervical lymph nodes.
The classic histologic findings of HVCD involve numerous regressed germinal centers with expanded mantle zones and a hypervascular interfollicular region. The germinal centers are predominantly follicular dendritic cells and endothelial cells. The mantle zone gives a concentric appearance, often being likened to an “onion skin” pattern. Blood vessels from the interfollicular area penetrate into the germinal center at right angles, giving rise to another food related identifier, “lollipop” follicles. A useful diagnostic tool is the presence of more than one germinal center within a single mantle zone.
The differential diagnosis of HVCD includes late stage HIV-associated lymphadenopathy, early stages AITL, follicular lymphoma, mantle cell lymphoma, and a nonspecific reactive lymphadenopathy. A history of HIV or diagnostic laboratory testing for HIV would exclude the first diagnosis. AITL usually presents histologically as a diffuse process but atypia in T-cells with clear cytoplasm that co-express CD10 and PD-1 outside of the germinal center are invariably present. EBER staining may reveal EBV positive B immunoblasts in early AITL, which would be absent in HVCD. The most challenging differential would include the mantle zone pattern of mantle cell lymphoma. Flow cytometry revealing a monotypic process with co-expression of cyclin D1 on IHC would further clarify the diagnosis.1
Overall, unicentric Castleman’s disease is usually of the hyaline vascular type. Surgical resection is usually curative in these cases with an excellent prognosis.2
References
- Jaffe, ES, Harris, NL, Vardiman, J, Campo, E, Arber, D. Hematopathology. Philadelphia: Elsevier Saunders, 2011. 1st ed.
- Ye, B, Gao, SG, Li, W et al. A retrospective study of unicentric and multicentric Castleman’s disease: a report of 52 patients. Med Oncol (2010) 27: 1171.

-Phillip Michaels, MD is a board certified anatomic and clinical pathologist who is a current hematopathology fellow at Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. His research interests include molecular profiling of diffuse large B-cell lymphoma as well as pathology resident education, especially in hematopathology and molecular genetic pathology.
