A patient presented to the Emergency Department at the St. Paul’s Hospital. Initial blood was collected by phlebotomy staff (one poke) at 6:55 am in the morning and the specimen was received in the lab at 7:11 am.
Emergency phoned the lab about these discrepant potassium results. What is going on?! The venous gas specimen was centrifuged and appeared hemolysed (3+), while the plasma sample had no evidence of hemolysis.
The phlebotomist indicated there was no problem with the collection. Repeat testing was initiated an hour later.
The venous gas specimen was centrifuged and appeared hemolysed (3+).
Because the venous gas specimens were transported on ice and the other tubes of blood collected were sent at room temperature, the biochemist discussed the possibility of a red cell cold agglutinin with the ER physicians. The ER physicians requested evaluation for a cold agglutinin (the EDTA tube collected for early hematology was used for this analysis). Lab staff performed the screen and it was 4+ for cold agglutinin. ER physicians were advised to believe the lower potassium results and to avoid sending further specimens on ice for this patient.
-Dr. Andrew Lyon, PhD, FCACB, DABCC is a clinical chemist and clinical toxicologist. He is the current past-president of the Canadian Society of Clinical Chemists. He is currently Division Head of Clinical Biochemistry of the Saskatoon Health Region and teaches general pathology residents as a clinical associate professor of Pathology and Laboratory Medicine at the University of Saskatchewan.
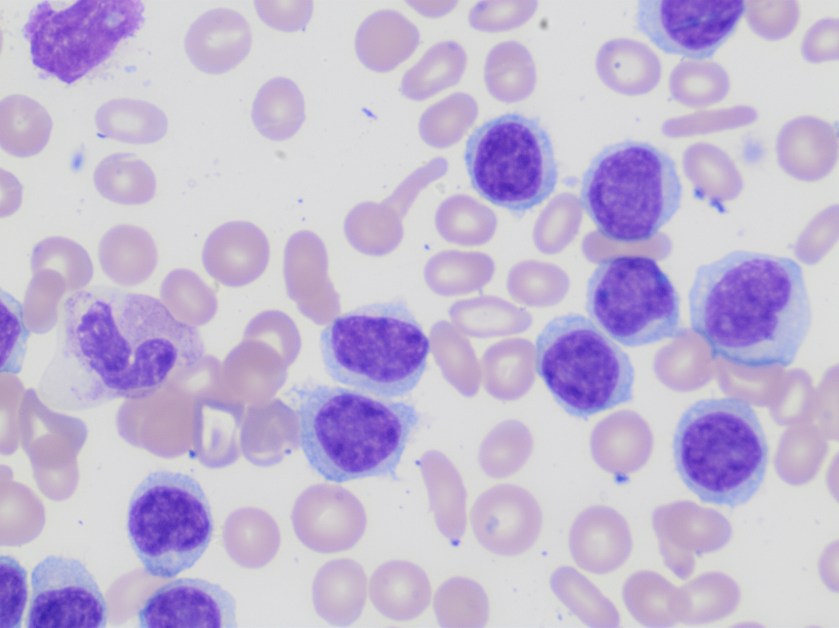
A 63 year old patient presented with a high white cell count of 108 K/uL and thrombocytopenia of 110 K/uL.
Peripheral smear examination revealed marked lymphocytosis with presence of numerous small to medium sized lymphoid cells with round to oval nuclei, clumped nuclear chromatin and variable amount of cytoplasm, some with cytoplasmic projections. As the features were consistent with a lymphoproliferative disorder peripheral blood was sent for flow cytometry.
Based on the morphology the differential diagnosis included B-cell lymphoproliferative disorders such as marginal zone lymphoma, hairy cell leukemia/variant, or less likely chronic lymphocytic leukemia and/or mantle cell lymphoma.
Flow cytometry revealed presence of clonal B-cells expressing CD19, CD20, Cd11c, CD103 and FMC-7. The cells were negative for CD5, CD10, and CD25.
The phenotype together with the morphology and CBC findings were diagnostic of hairy cell leukemia variant.
Discussion
Hairy cell leukemia variant ( HCL-v) is a B-cell lymphoproliferative disorder that resembles classic hairy cell leukemia but exhibits variant cytological and hematological features such as leukocytosis and also shows variant immunophenotype including absence of CD25, CD123 and/or annexin A1.
HCL-v is about one tenth as common as HCL (hairy cell leukemia) with an annual incidence of approximately 0.03 cases per 100,000 population. There is slight male preponderance. Patients with HCL-v typically present with leukocytosis with an average WBC of 30 K/ul and /or thrombocytopenia.
The 5 year survival rate is around 50-60%. Most patients require therapy which can range from splenectomy to combination chemotherapy with Rituximab.
Reference
WHO classification of Tumors of Haematopoietic and Lymphoid Tissues; IARC 2017
-Neerja Vajpayee, MD, is the director of Clinical Pathology at Oneida Health Center in Oneida, New York and is actively involved in signing out surgical pathology and cytology cases in a community setting. Previously, she was on the faculty at SUNY Upstate for several years ( 2002-2016) where she was involved in diagnostic work and medical student/resident teaching.
A 74 year old female presented to the ED with a chief complaint of fever, right knee swelling and pain for three days. Past medical history was significant for a right total knee arthroplasty approximately 5 months prior, with no significant complications. Physical exam revealed the patient to be febrile (103 degrees Fahrenheit), a swollen right knee that was warm to the touch and erythema surrounding the surgical incision site. Routine labs were obtained while in the ED which revealed a leukocytosis with an elevated ESR and CRP. Imaging was ordered and showed a large joint effusion of the right knee with intact hardware. Arthrocentesis was performed which returned 80 cc of cloudy yellow fluid with no crystals identified by light microscopy, a nucleated cell count of 169,200/cmm of which 97% were neutrophils.
Laboratory Identification
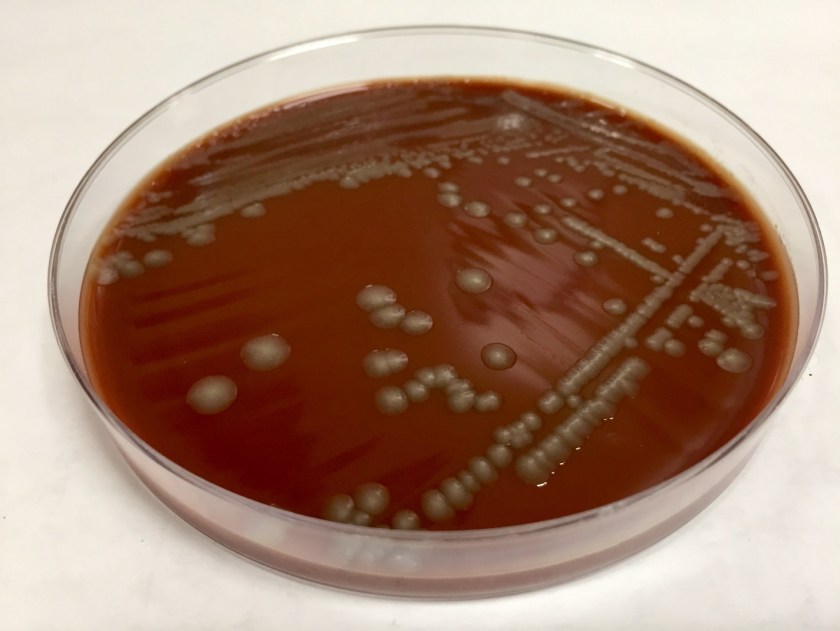
The primary gram stain was reported as polys and gram negative bacilli present. Cultures revealed a pure moderate growth on sheep blood and chocolate agar with no growth on the MacConkey agar. Colony morphology on the sheep blood agar was smooth, gray with no hemolysis appreciated. The key biochemical and physiologic characteristics of the isolate included: positivity for indole, nitrate reduction, catalase, ornithine decarboxylase, and fermentation of mannitol and sucrose; negativity for urea and maltose fermentation. The isolate was identified by MALDI-TOF as Pasteurella multocida. Upon further questioning, the patient admitted to living with two indoor cats but denied any recent history of bites or scratches.
Image 1. Chocolate agar with smooth gray colonies.
Discussion
Pasteurella multocida is a non-motile, oxidase positive, small -gram negative bacilli capable of fermenting glucose. This organism is part of the normal flora of the gastrointestinal tract and nasopharynx of wild and domestic animals. Humans who have extensive exposure to animals may be found to have Pasteurella multocida as part of their upper respiratory tract flora. With no significant virulence factors, this organism is often viewed as an opportunistic pathogen which requires mechanical disruption of anatomic barriers as occurs with bite and scratch wounds from cats and dogs. Though most infections are associated with bites or scratched from animals, infection can occur with non-bite exposure to animals. The typical disease caused by Pasteurella multocida is a focal soft tissue infection following a bite or scratch. However, chronic respiratory infections in patients with preexisting chronic lung disease and heavy animal exposure, and bacteremia with metastatic abscess formation have been documented.
Biochemical characteristics can be utilized in identifying the different Pasteurella species. The key biochemical and physiologic characteristics for Pasteurella multocida include: positivity for indole, nitrate reduction, catalase, ornithine decarboxylase, and fermentation of mannitol and sucrose; negativity for urea and maltose fermentation.
The vast majority of these organisms are susceptible to penicillin, thus susceptibility testing is generally unnecessary. Additionally, soft tissue infections caused by animal bites are frequently polymicrobial and warrant use of therapeutics with a broader spectrum. However, should the need arise to perform susceptibility testing, the Clinical and Laboratory Standards Institute (CLSI) does provide break points for Pasteurella multocida.
Koneman EW. Koneman’s Color Atlas and Textbook of Diagnostic Microbiology. Lippincott Williams & Wilkins; 2006.
-Justin Rueckert, DO is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.