Case History
A 63 year old patient presented with a high white cell count of 108 K/uL and thrombocytopenia of 110 K/uL.
Peripheral smear examination revealed marked lymphocytosis with presence of numerous small to medium sized lymphoid cells with round to oval nuclei, clumped nuclear chromatin and variable amount of cytoplasm, some with cytoplasmic projections. As the features were consistent with a lymphoproliferative disorder peripheral blood was sent for flow cytometry.
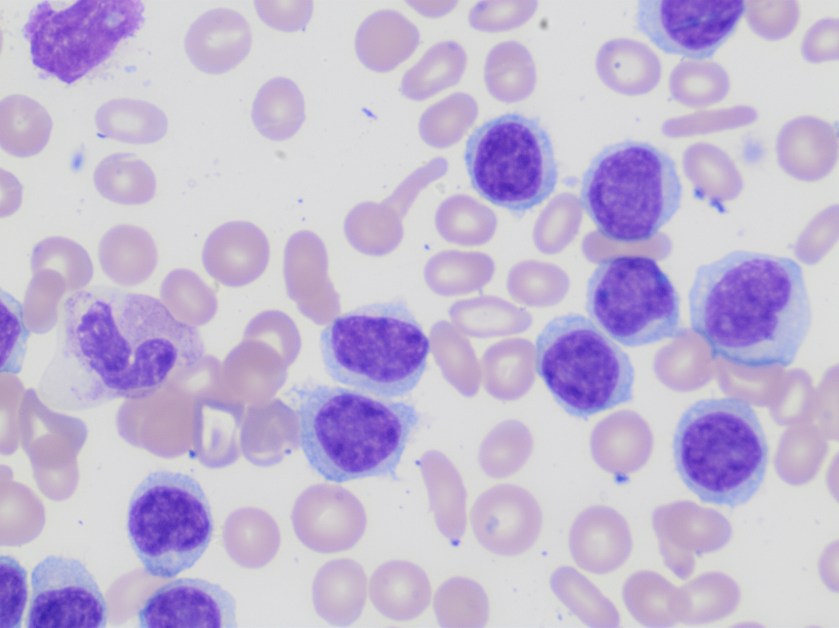

Based on the morphology the differential diagnosis included B-cell lymphoproliferative disorders such as marginal zone lymphoma, hairy cell leukemia/variant, or less likely chronic lymphocytic leukemia and/or mantle cell lymphoma.
Flow cytometry revealed presence of clonal B-cells expressing CD19, CD20, Cd11c, CD103 and FMC-7. The cells were negative for CD5, CD10, and CD25.
The phenotype together with the morphology and CBC findings were diagnostic of hairy cell leukemia variant.
Discussion
Hairy cell leukemia variant ( HCL-v) is a B-cell lymphoproliferative disorder that resembles classic hairy cell leukemia but exhibits variant cytological and hematological features such as leukocytosis and also shows variant immunophenotype including absence of CD25, CD123 and/or annexin A1.
HCL-v is about one tenth as common as HCL (hairy cell leukemia) with an annual incidence of approximately 0.03 cases per 100,000 population. There is slight male preponderance. Patients with HCL-v typically present with leukocytosis with an average WBC of 30 K/ul and /or thrombocytopenia.
The 5 year survival rate is around 50-60%. Most patients require therapy which can range from splenectomy to combination chemotherapy with Rituximab.
Reference
- WHO classification of Tumors of Haematopoietic and Lymphoid Tissues; IARC 2017

