Case History
A 56-year-old male with a past medical history significant for HIV currently on HAART presented to his primary care physician with an isolated enlarged left inguinal lymph node. In the context of his immunocompromised state, the patient was sent for a core needle biopsy of the lymph node to further elucidate the etiology of the isolated lymphadenopathy.
Diagnosis
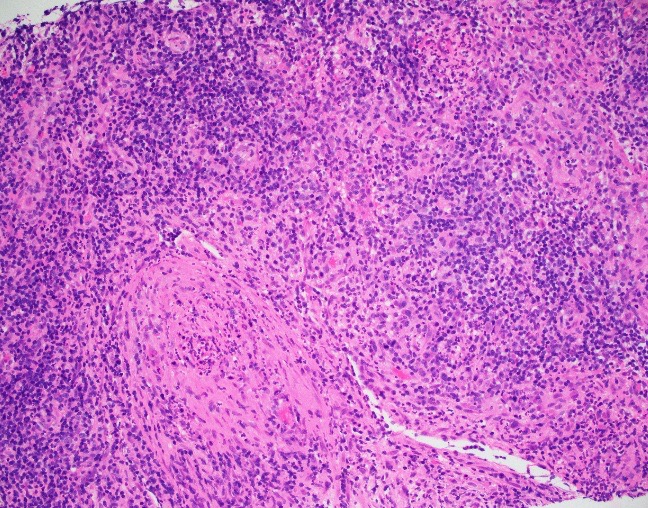



The core needle biopsy demonstrated multiple suppurative granulomata with a mixed inflammatory background including abundant plasma cells. The plasma cells are also found to surround small blood vessels. A Treponema immunostain was performed which highlighted the spirochetes. Overall, the diagnosis is that of luetic lymphadenitis.
Discussion
Syphilitic infections can cause isolated lymphadenopathy, especially in the inguinal lymph nodes. The morphologic features of luetic lymphadenitis include interfollicular plasmacytosis, capsular fibrosis, endarteritis, and occasionally sarcoid-like granulomata with rare cases demonstrating suppurative features. The differential diagnosis includes rheumatoid arthritis associated lymphadenopathy but a key histologic difference is that the capsular fibrosis of luetic lymphadenitis will have an infiltrate of lymphocytes and plasma cells while RA associated lymphadenopathy traditionally does not. Immunohistochemistry for Treponema organisms also serves to confirm the diagnosis. It is important to keep in mind the patient’s clinical history when interpreting the biopsy was as well as the differential for interfollicular plasmacytosis with capsular fibrosis.

-Phillip Michaels, MD is a board certified anatomic and clinical pathologist who is a current hematopathology fellow at Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. His research interests include molecular profiling of diffuse large B-cell lymphoma as well as pathology resident education, especially in hematopathology and molecular genetic pathology.

Interesting case and discussion. If the patient’s history were not known, would the diagnoses be different, or simply more revealing?
The diagnosis would be unchanged and would most definitely be revealing. The clinician was not expecting this and the patient was treated accordingly.