Clinical history
A 65 year old man with diabetes mellitus type 2 presented to the emergency department (ED) for left hip pain. He has a remote history of avascular necrosis of bilateral hips of unknown etiology for which he received a bilateral total hip arthroplasty and subsequent multiple revisions due to hardware failure several years ago. He initially presented to an urgent care clinic a few months prior for “noise with movement” of the left hip and mild lower back pain. Plain radiographs of the left hip in comparison to his prior imaging were unremarkable and he was subsequently discharged. Repeat imaging at a follow-up visit at the orthopedic clinic showed mild superior migration of the femoral head bilaterally secondary to periprosthetic osteolysis of the joint headliner. He was scheduled for surgery however presented to the ED prior to his scheduled appointment with severe crushing left hip pain and restricted joint mobilization. He denied fevers, chills, night sweats, or any other recent infections. The left hip was aspirated yielding 10cc of dark black fluid and a stat gram stain was ordered.
Laboratory identification
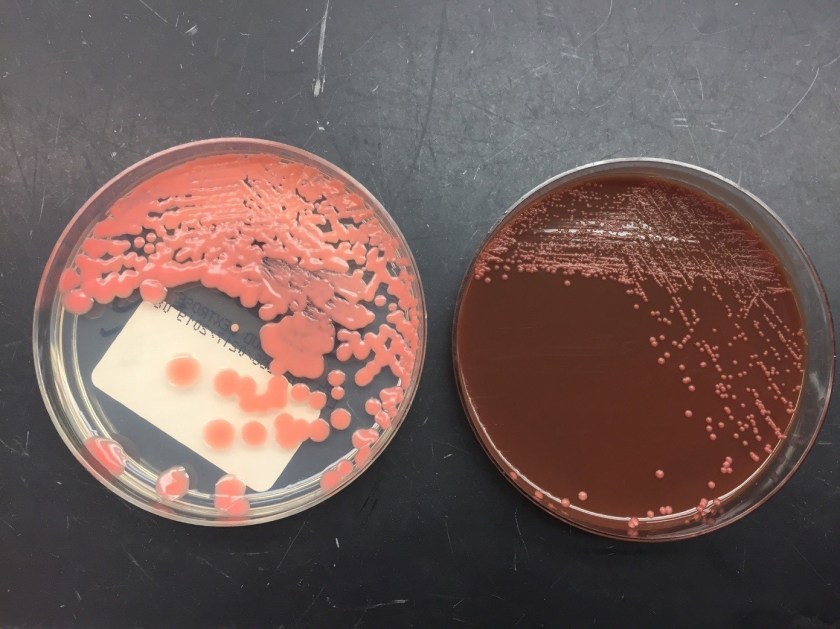
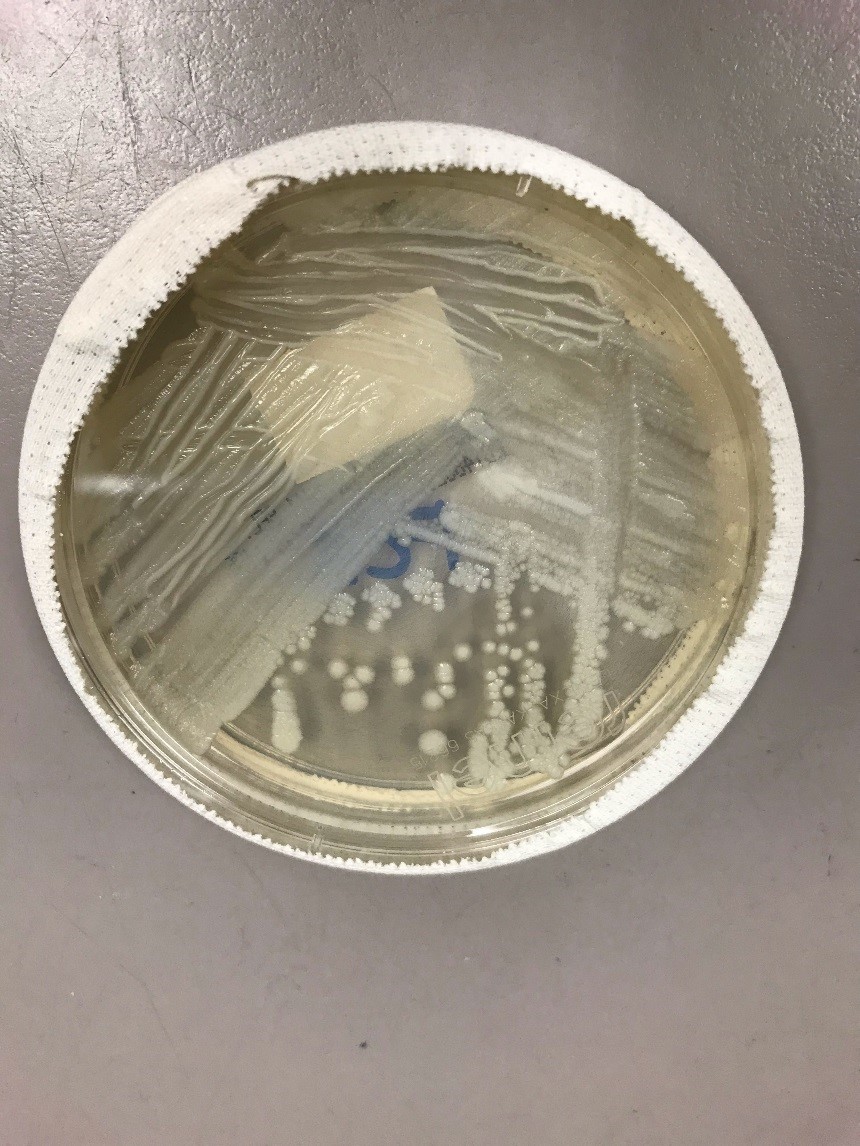
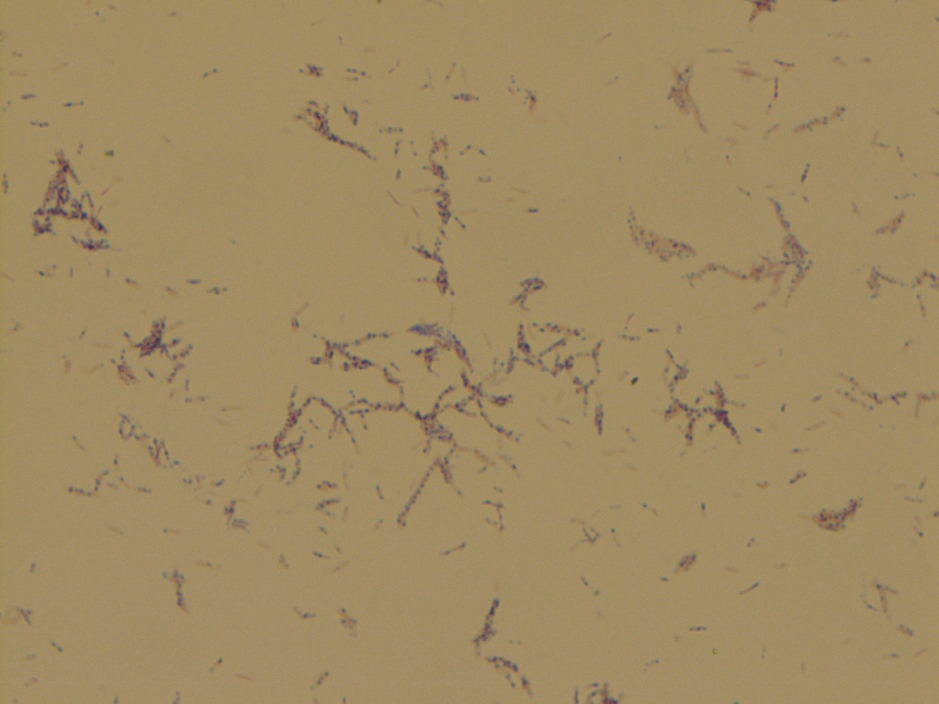
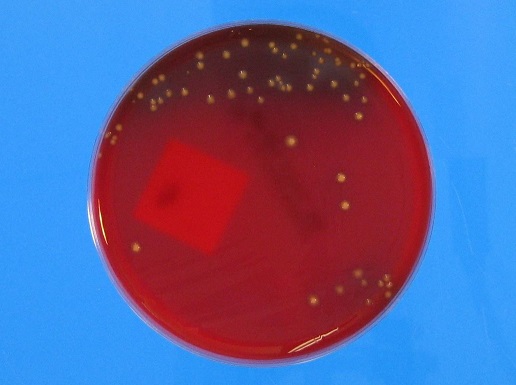
The stat gram stain showed many polymononuclear cells with moderate gram positive bacilli in a background of dark inorganic material (Image 1). Following 48 hours of incubation, there was anaerobic growth on the kanamycin and vancomycin (KV) and schaedler agar plates. A Gram stain of the broth showed gram positive bacilli arranged singly and in chains with some decolorization (Image 2). The KV and schaedler plates showed moderate growth of a single organism consisting of small glossy tan colored colonies (Images 3-4). No aerobic growth was observed on the blood, MacConkey, Columbia Naladixic Acid (CNA), or chocolate agar plates. Mass spectrometry (MALDI-TOF) identified the pathogenic organism as Clostridium innocuum.



Discussion
Bacterial joint infections are more common in prosthetic joints as compared to native joints with a prevalence of 1-2% following hip arthroplasty (1). Most cases of bacterial septic arthritis are due to staphylococci (40 percent), streptococci (28 percent) or gram negative bacilli (19 percent) organisms (2). Joint infections secondary to anaerobes are less likely and account for 2-3% of all cases (3). A review of the literature shows less than 50 documented cases of septic arthritis due to Clostridium species. Amongst these cases Clostridium perfringens is the most commonly isolated pathogen (4). To date there are no documented cases of joint infections secondary to Clostridium innocuum species.
Clostridium innocuum is a non-motile, anaerobic, gram positive organism that reproduces by sporulation. These organisms are normally found as a part of the usual human gut flora and are rarely human pathogens. The name “innocuum” is derived from the term “innocuous” to convey the innocence of these organisms as they do not produce clostridial exotoxins. A review of the literature shows fewer than 20 reported cases of Clostridium innocuum infections with most reported cases being described in immunocompromised patients such as those with diabetes mellitus, chronic hepatitis, acquired immune deficiency syndrome (AIDS), leukemia, and organ transplantation (5-6). Clinically patients can present with a spectrum of symptoms which include fever of unknown origin, diarrhea/constipation, and non-specific respiratory symptoms. In almost all cases bacteremia ensued. Most cases were associated with a traumatic penetrating injury with few reported cases due to hematogenous spread (5-6).
Laboratory identification of Clostridium innocuum can be challenging due to its variable gram staining morphology and atypical colony morphology on differing culture media. Most traditional phenotypic methods can only reliably identify these organisms to the genus level as a Clostridium species. However, using mass spectrometry (MALDI-TOF) these organisms can be identified to the species level. Rapid identification of Clostridium innocuum from the subset of Clostridium species is clinically important as these organisms are the only known Clostridium species with intrinsic resistance to vancomycin (7). Although they do not possess clostridial exotoxins, these organisms are thought to have a lipopolysaccharide-like virulence factor and have a mortality rate comparable to toxigenic Clostridium species (7). Due to resistance to vancomycin, metronidazole, piperacillin and ampicillin-sulbactam are the alternative recommended first-line treatment options.
For this patient, following the results of the gram smear the patient was started on IV vancomycin but due to an adverse allergic reaction was switched to intravenous pencillin G and oral ciprofloxacin. He was subsequently taken to the operating room for incision and drainage and left hip revision arthroplasty with cup exchange. Blood cultures were collected post-operatively and showed no growth, possibly due earlier antibiotic administration. Susceptibility studies from Mayo Laboratories showed pan susceptibility to penicillin, piperacillin-tazobactam, ertapenem, clindamycin, and metronidazole. The patient was subsequently switched to intravenous penicillin and continued to show clinical improvement during his remaining hospital course.
References
- Horowitz DL, Katzap E, Horowitz S, Barilla-labarca ML. Approach to septic arthritis. Am Fam Physician. 2011;84(6):653-60.
- Ryan MJ, Kavanagh R, Wall PG, Hazleman BL. Bacterial joint infections in England and Wales: analysis of bacterial isolates over a four year period. Br J Rheumatol. 1997;36(3):370-3.
- Shah NB, Tande AJ, Patel R, Berbari EF. Anaerobic prosthetic joint infection. Anaerobe. 2015;36:1-8.
- Gredlein CM, Silverman ML, Downey MS. Polymicrobial septic arthritis due to Clostridium species: case report and review. Clin Infect Dis. 2000;30(3):590-4.
- Leal J, Gregson DB, Ross T, Church DL, Laupland KB. Epidemiology of Clostridium species bacteremia in Calgary, Canada, 2000-2006. J Infect. 2008;57(3):198-203.
- Lee NY, Huang YT, Hsueh PR, Ko WC. Clostridium difficile bacteremia, Taiwan. Emerging Infect Dis. 2010;16(8):1204-10.
- Chia JH, Feng Y, Su LH, et al. Clostridium innocuum is a significant vancomycin-resistant pathogen for extraintestinal clostridial infection. Clin Microbiol Infect. 2017;23(8):560-566.
-Noman Javed, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.