Case Description
A 69 year old man with hepatitis B and chronic cutaneous Rosai-Dorfman disease presented to the dermatology clinic for regular follow-up. He was being treated with subcutaneous injection of methotrexate every other week and intralesional Kenalog (ILK) injections for individual lesions. The patient presented with a new complaint of a painful nodule on his left thumb where he was stuck with a splinter two months prior. He denied fever, chills, weight loss, or other systemic symptomology. Upon physical examination, an erythematous nodule on the lateral left thumb with central pallor and crusting consistent with a foreign body was observed (Figure 1). Surgical excision was recommended.

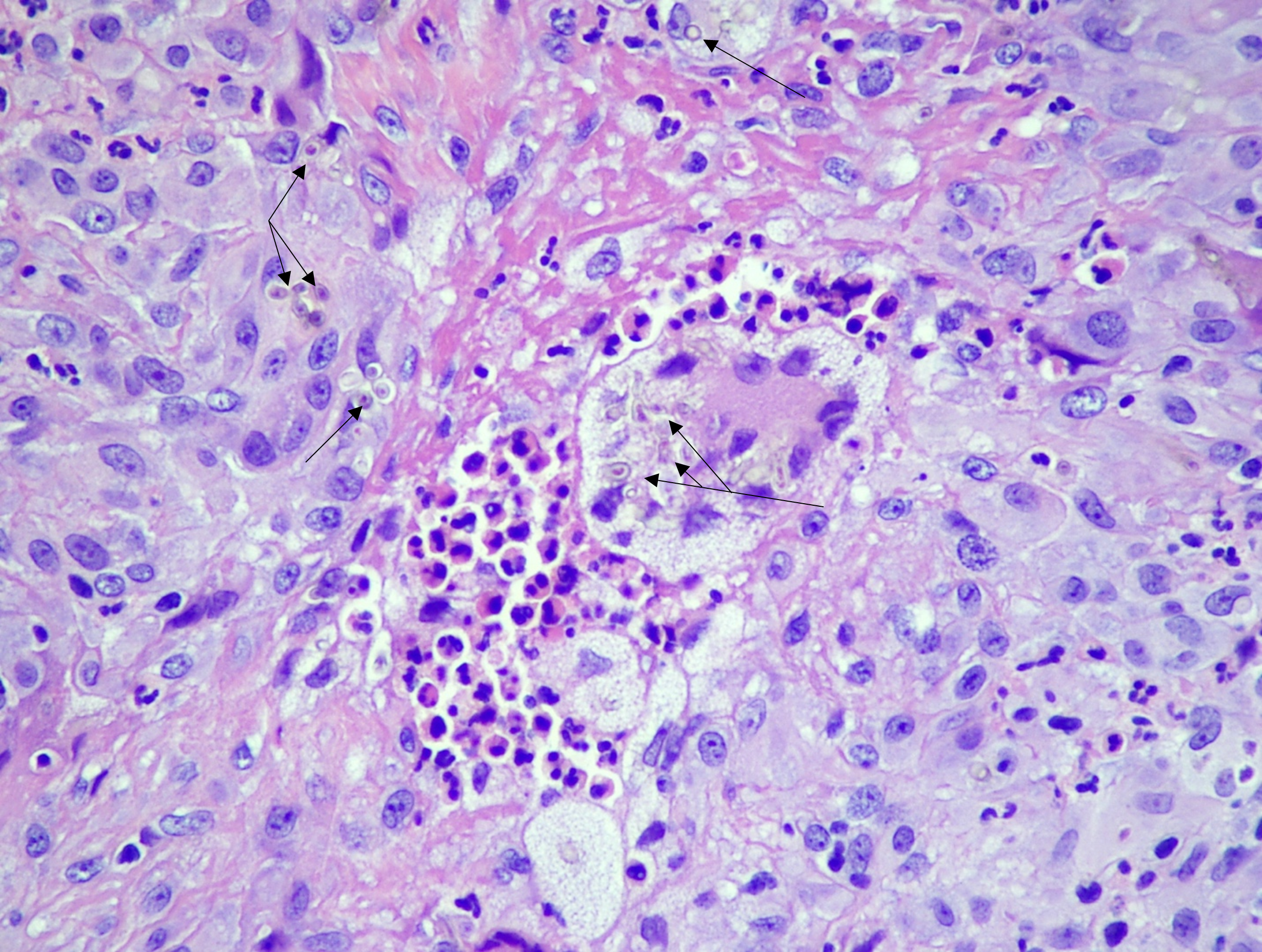
Following excisional biopsy, histopathology revealed a relatively circumscribed lesion with suppurative granulomatous dermatitis and numerous pigmented hyphae observed on hematoxylin and eosin stained slides (H&E; [Figures 2-3]). A diagnosis of phaeohyphomycosis was made; the patient’s methotrexate was held and an infectious disease (ID) consult was placed. Precautionary blood cultures were drawn which remained negative following five days of incubation. The patient was started on a course of empiric oral doxycycline for two weeks which he completed. At presentation for ID follow up, the patient felt well and denied constitutional symptoms or recurrence of the thumb lesion. Physical exam revealed no associated sporotrichoid lesions (lymphocutaneous spread of infection) or palpable lymphadenopathy. ID recommended a 3-month course of oral itraconazole as secondary prophylaxis, which was completed without adverse effects or recurrence of symptoms.

Case Discussion
Phaeohyphomycosis describes a constellation of clinical syndromes caused by infection with a broad group of “dematiaceous” or “melanized” molds and some pigmented yeasts.1 Many of these organisms are ubiquitous in the environment though some are more selective in their habitat, restricting the likelihood of infection to specific geography or select patient populations.2,3 Despite significant microbiological diversity, a unifying characteristic of dematiaceous molds is the production of the pigment melanin. Melanin is theorized to serve as a virulence factor, as loss of melanization often results in attenuation.3,4 In contrast to other diseases caused by dematiaceous molds with more defined etiologies and presentations (e.g., eumycetoma, chromoblastomycosis), manifestations of phaeohyphomycosis are highly variable and can include keratitis, cutaneous disease, pulmonary infection, central nervous system penetration and/or disseminated disease.
Laboratory diagnosis of phaeohyphomycosis is reliant on histopathological evaluation, as surgical debridement is often necessary for management. In this setting, darkly pigmented, septate hyphae invading tissue in a nonspecific background of inflammation may be observed.1 H&E staining is generally sufficient to confirm diagnosis; however, special stains that can highlight fungi, namely Grocott-Gomori methenamine silver (GMS) or periodic acid-Schiff (PAS) stains, can outline the presence of hyphal elements. Additionally, melanin production can be highlighted using Fontana-Masson staining. Careful evaluation and interpretation of fungal cultures, when collected, are important as results can be complex given the ubiquitous nature of many etiological agents, particularly from non-sterile anatomical sites. Additionally, there are no alternate methods routinely available to aid in diagnosis, outside of culture, to specifically identify etiologic agents of phaeohyphomycosis.3 Importantly, optimal antifungal therapy for these infections remains unclear due to a lack of randomized control trials and relative infrequency of presentation.
Superficial infections, such as the one described in this case, are generally considered to be consequences of local trauma, and exhibit minimal tissue invasion. However, in the setting of the immunocompromised host or immunosuppression, disseminated infection can occur.3 The prognosis of invasive phaeohyphomycosis is poor, exhibiting a mortality is as high as 10% for deep local infections and 50% for disseminated disease.1 This patient’s advanced age and chronic immunosuppression were cause for great concern. Fortunately, the biopsy demonstrated granuloma formation effectively localizing the infection to the subcutaneous tissue of the thumb. The patient has remained free of further disease to date, suggestive of a curative surgical resection.
References
- Arcobello, JT, Revankar, SG. Phaeohyphomycosis. Respiratory and Critical Care Medicine. 2020. DOI: 10.1055/s-0039-3400957
- Wong EH, Revankar SG. Dematiaceous Molds. Infectious Disease Clinics of North America. 2016. 10.1016/j.idc.2015.10.007
- Revankar, SG., Baddley, JW., Chen, S.C-A., Kauffman, CA., Slavin, M., Vazquez, JA, Seas, C., Morris, MI., Nguyen, MH et. al. A Mycoses Study Group International Prospective Study of Phaeohyphomycosis: and Analysis of 99 Proven/Probable Cases. Open Forum Infectious Diseases. 2017. DOI: 10.1093/ofid/ofx200
- Sharkey PK, Graybill JR, Rinaldi MG, Stevens DA, Tucker RM, Peterie JD, Hoeprich PD, Greer DL, Frenkel L, Counts GW, et al. Itraconazole treatment of phaeohyphomycosis. Journal of the American Academy of Dermatology. 1990. doi: 10.1016/0190-9622(90)70259-k
-Kevin Burningham is a 4th year medical student at UT Southwestern Medical School.
-Dominick Cavuoti is a Professor at UT Southwestern Medical Center who specializes in Cytopathology, Infectious Disease pathology and is a medical director of the Microbiology laboratory at Parkland Health and Hospital System.

-Clare McCormick-Baw, MD, PhD is an Assistant Professor of Clinical Microbiology at UT Southwestern in Dallas, Texas. She has a passion for teaching about laboratory medicine in general and the best uses of the microbiology lab in particular.

-Andrew Clark, PhD, D(ABMM) is an Assistant Professor at UT Southwestern Medical Center in the Department of Pathology, and Associate Director of the Clements University Hospital microbiology laboratory. He completed a CPEP-accredited postdoctoral fellowship in Medical and Public Health Microbiology at National Institutes of Health, and is interested in antimicrobial susceptibility and anaerobe pathophysiology.
