Case History
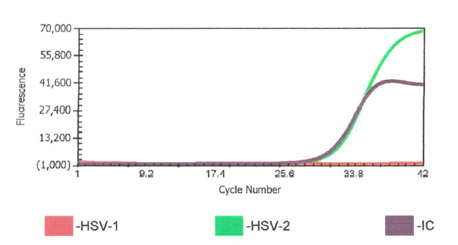
The patient was a previously healthy female who presented with a five day history of retro-orbital headaches, lightheadedness, and intermittent falls. Her presentation was consistent with meningitis and further studies were pursued. Head computed tomography (CT), CT angiogram of the head and neck, brain magnetic resonance imaging (MRI), and electroencephalogram (EEG) were unremarkable. Analysis of the cerebrospinal fluid (CSF) demonstrated an elevated white blood cell count (605 white blood cells/µL) of which 88% were lymphocytes, 9% were monocytes, and 3% were neutrophils. CSF glucose was slightly decreased at 33 mg/dL and protein was elevated at 81 mg/dL. Additional tests requested on the CSF included herpes simplex virus (HSV), varicella zoster virus (VZV), West Nile virus (WNV), and Epstein-Barr virus (EBV). The CSF was positive for HSV-2 and negative for HSV-1, VZV, and EBV by PCR. WNV IgG and IgM were negative. Of note, the patient had two episodes of viral meningitis in the past of unknown etiology. The patient received a one week course of valacyclovir and was discharged. Per the patient, she continues to have fluctuating headaches and occasional lightheadedness. Follow-up imaging has been unremarkable.
Discussion
Herpes simplex virus 1 and 2 (HSV-1 and HSV-2) are enveloped, double stranded DNA viruses that are members of the Herpesviridae family. They are common viruses that cause cold sores or fever blisters. HSV is a lifelong infection, and latent infection can cause reactivation. While both HSV-1 and HSV-2 can affect any area, HSV-1 is typically associated with non-genital sites whereas HSV-2 typically causes genital infections. In addition to herpetic gingivostomatitis, herpes labialis, and herpes genitalis, other associated clinical conditions include encephalitis, meningitis, keratitis, esophagitis, neonatal herpes, and disseminated primary infection. Most cases of HSV encephalitis have been linked to HSV-1 while HSV meningitis is typically caused by HSV-2. As seen in our patient, HSV-2 has been implicated in recurrent, aseptic, and self-limiting meningitis, also known as Mollaret meningitis.1 There are no specific treatment guidelines for HSV-2 meningitis with the main therapeutic strategy being symptom management. The utilization of acyclovir to manage uncomplicated HSV-2 management is controversial and there is no current consensus.2
Clinically, patients with meningitis typically present with acute onset of fever, headache, and neck stiffness. Other associated symptoms include malaise, rash, nausea, vomiting, sore throat, lymphadenopathy, and genitourinary symptoms. In order to differentiate between the infectious etiologies (i.e. viral, bacterial, tuberculous, or fungal) that cause meningitis, a lumbar puncture may be performed. For viral meningitis, CSF will usually show an elevated white count with predominantly mononuclear cells. The CSF:serum glucose ratio and protein levels are often elevated. The most common CSF viral pathogens in the non-immunosuppressed population are enteroviruses, HSV-1, HSV-2, and VZV, which can all be detected by real time polymerase chain reaction (RT-PCR) technology Molecular methods are faster, more sensitive, and more widely available that viral culture.3 Antibody tests are not recommended for HSV as ~70% of adults will be positive for HSV-1 and ~20-50% of adults will be positive for HSV-2.4
Given the broad range of infectious etiologies that can cause meningitis, there has been interest in the development of a multiplex molecular test. Currently, the FilmArray meningitis/encephalitis panel is the only one that has received FDA clearance. This panel includes 14 bacterial, fungal, and viral targets, including HSV-1 and HSV-2. However, this panel should be used cautiously as several studies have shown a high proportion of false negatives in the detection of HSV-1, HSV-2, and Crytococcus neoformans/gattii. It has been suggested that for HSV-1 and HSV-2, the multiplex panel does not work as well if the viral load is near the limit of detection of the assay or if the patient is having a reactivation of HSV. If there is a high clinical suspicion, particularly in neonates and immunosuppressed patients, an assay for detection of only HSV-1 and HSV-2 should be performed.5
References
- Koelle DM and Corey L. (2008) Herpes simplex: insights on pathogenesis and possible vaccines. Annual Review of Medicine, 59: 381-395.
- Bamberger DM. (2010) Diagnosis, initial management, and prevention of meningitis. American Family Physician, 82: 1491-1498.
- Logan SAE and MacMahon E. (2008) Viral meningitis. The BMJ, 336: 36-40.
- Schiffer JT, Corey L. (2020) Herpes simplex virus. Bennett’s Principles and Practice of Infectious Diseases, 9th edition.
- Tansarli GS and Chapin KC. (2020) Diagnostic test accuracy of BioFire FilmArray meningitis/encephalitis panel: a systematic review and meta-analysis. Clinical Microbiology and Infection, 26: 281-290.

-Melissa Tjota, MD, PhD is a Molecular Genetic Pathology fellow at the University of Chicago Medicine and NorthShore University HealthSystem. She completed her MD/PhD (Immunology) and AP/CP residency at the University of Chicago.

-Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
