Now that you’ve seen some malignant ocular entities (both primary and metastatic), I’d like to share some (in my eyes) curveballs. Working in a cancer center, I see more cancer than I do benign processes. You can say I’m fine tuned to identifying malignant cells, and I find it difficult to rest assured that what I’m diagnosing truly is benign. When you find one malignant cell in a pleural fluid, changing the patient’s diagnosis from Stage II to Stage IV, that primed search for atypia is always on. With that said, not every specimen screened at a cancer center is malignant. We rule out malignancy and confirm benign processes as well. As for benign ocular FNAs, well… you have to be as certain calling benign as you do malignant because the process of acquiring an additional sample to confirm your diagnosis is just as involved and unpleasant as the first biopsy.
Here, I present six non-malignant eye FNA cytopreparations that had me searching for atypia longer than I expected.
Case 1. A 72 year old female with a history of breast carcinoma; She presented with a choroidal nevus, OD in 2014. The oncologist noted a slight increase in base and thickness six years after the initial evaluation. The clinical diagnosis is a choroidal nevus, rule out low-grade melanoma.

Final Diagnosis: No malignant cells identified. A few benign-appearing melanocytes, consistent with nevus.
Note: Material is scant cellular and consists mainly of scattered retinal pigment epithelial cells and sensory cells. There are a few benign-appearing spindle-shaped cells with bland nuclei, consistent with nevus. However, the paucity of the sample precludes a definitive diagnosis. Recommend clinical correlation to exclude sampling error.
Case 2. A 21 month old male with a history of an iris stromal cyst, OS. Lesion is status post-FNA (twice), had regrowth, and aspirated for the third time. Previous FNAs showed no malignant cells.
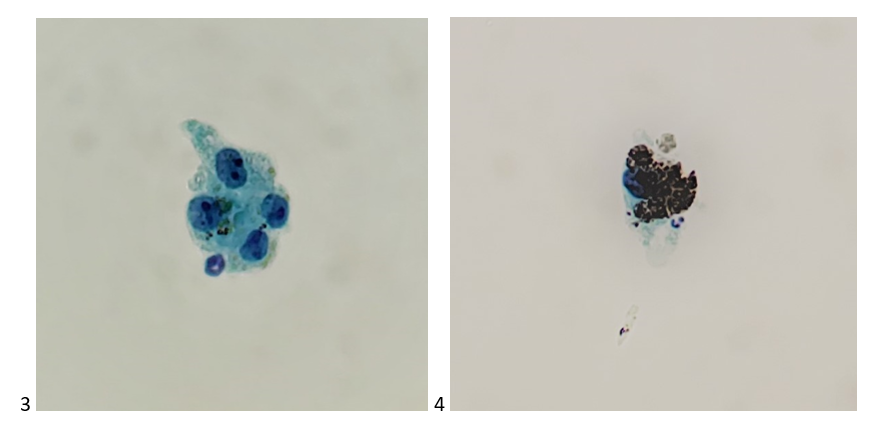
Final Diagnosis: No malignant cells identified. Rare pigment-laden macrophages, a few lymphocytes, and benign surface epithelial cells present. (Consistent with stromal cyst).
Case 3. A 65 year old female with a history of nevus, OD. Ocular oncology followed up and noted an increase in thickness from 2.76 to 3.00 mm. In light of family history of cutaneous melanoma, treatment is suggested. Clinical diagnosis: ciliary body melanoma.

Final Diagnosis: Scant mildly atypical amelanotic spindle cells, consistent with nevus.
Note: Diagnostic material is very scant. There are a few benign-appearing single spindle cells and one cluster of cohesive spindle cells with no pigment. Prominent nucleoli are not seen. While the cytologic features in the context of clinical presentation is consistent with nevus, the paucity of the sample precludes a definitive diagnosis. There is no diagnostic evidence of malignant melanoma in this sample. Recommend clinical correlation to exclude sampling error.
Case 4. A 9 year old female with a history of retinoblastoma, OD; status post IAC (intra-arterial chemotherapy) x5, IVit melphalan x 4, and plaque radiotherapy. She recently developed vitreous hemorrhage (OD). Since the hemorrhage is obscuring the retinal view, vitrectomy is planned.
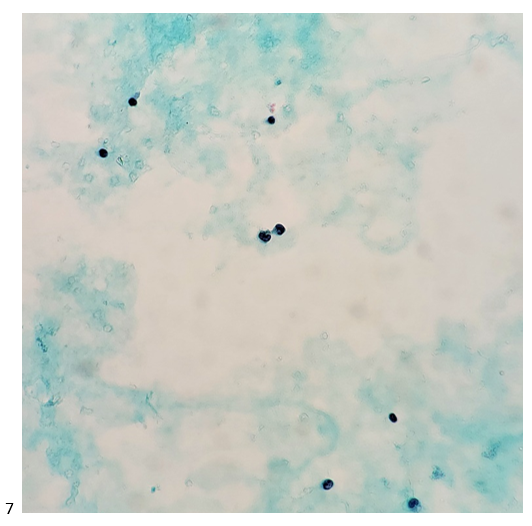
Final Diagnosis: No malignant cells identified. Lymphocytes and histiocytes present.
Case 5. An 11 year old female with vitreal retinoblastomas, OU; status post CRD therapy x6; plaque I-125, EBRT, proton beam; IVit Metphalan x2, and PPV (pars plana vitrectomy), OS. She now presents with dense vitreous hemorrhage blocking view since 2019.

Final Diagnosis: No malignant cells identified. Proteinaceous material and scattered small lymphocytes present.
Case 6. A 52 year old female with no cancer history. In 2019, she presented with pain, floaters, decreased visual acuity, and photophobia, OS. She was treated with antibiotic drops and steroids. In 2020, she was noted to have panuveitis with yellow iris nodules. FNA showed necrotic cells inadequate for diagnosis, as well as a negative culture and PCR for HSV, toxoplasmosis, CMV, and VZV. Clinical diagnosis: suspicious for iris lymphoma, OS.
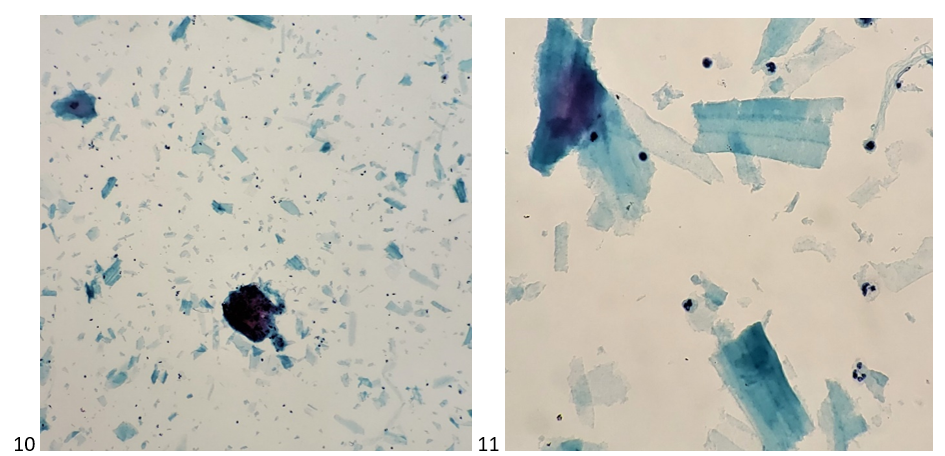
Final Diagnosis: Mixed inflammatory cells, favor an inflammatory process.
Note: There are neutrophils, lymphocytes, and scattered histiocytes in a background of numerous fragments of an amorphous substance. The cellularity is inadequate for flow cytometric analysis. We performed immunocytochemical stains on cytospin preparations. The lymphocytes are predominantly T-cells showing positive staining for CD45 and CD3 and negative for CD20. There is no diagnostic evidence of malignant lymphoma in this sample. The amorphous substance may represent lens fragments, in which case the possibility of lens-induced uveitis should be considered in the differential diagnosis. Recommend clinical correlation.
As you can tell, benign processes are complicated and require thorough explanations in our pathologic diagnoses, especially when they differ from the clinical impression. The majority of benign ocular FNAs are paucicellular, and we make the most of what we have through optimal preservation and preparation of cellular material. And don’t forget-not everything is cancer. Cyst contents, proteinaceous debris, and inflammatory cells make up a share of cases we see, and it’s okay to diagnosis them as benign. Just keep an eye out.

-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
