I left for vacation at the beginning of June thinking “once I get back, all of this COVID stuff will be quieted down.” …Well that wasn’t quite the case and testing for novel Coronavirus has continued to be very important. In fact, this last weekend I was tested by occupational health. It came back negative, but I’m am very enthusiastic to get alternative specimen types validated; those Nasopharyngeal swabs are quite…uncomfortable. Luckily, my test was processed at our institution which gets results back in 24-48 hours. However, with the resurgence around the country, turnaround times are backing up to 7-8 days. One solution has been the widely used IDNOW point of care platform. However, there has been significant concern over false negatives produced by this platform. One reason the sensitivity is different is because this platform performs isothermal amplification of nucleic acid. This method amplifies RNA at a stable temperature instead of cycling the temperature as in real-time PCR.
Colleagues at my institution reflexed any negative IDNOW samples to the m2000 Real-Time PCR assay for SARS-CoV-2 for one month. Within that time, over 500 samples were tested and the IDNOW was found to have missed 21% of positive cases (prevalence rate of 5%)2. One the positive side, it had a 98% negative predictive value, which helped rule out COVID19 infection. However, as prevalence rates are increasing, a high negative predictive value isn’t as important as sensitivity.
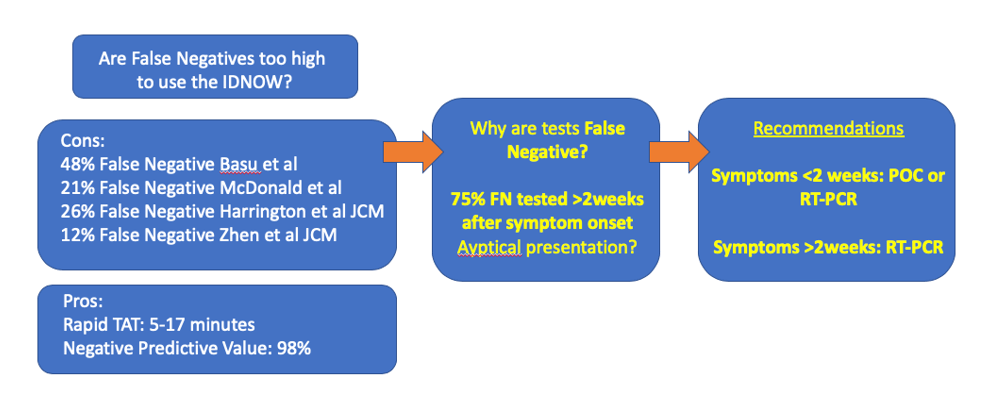
One study drew much attention when it claimed the IDNOW had a sensitivity of 52% in a New York City academic institution (Basu)4. However, this seems to be an outlier compared to other studies of this platform: one large multi-center study found positive percent agreement (equivalent of sensitivity when a gold standard test hasn’t been established) of 74%1. The highest PPA of 88%3 for the IDNOW was found in a study that indicated it can be completed in 17 minutes, whereas another quick instrument (but not point of care instrument: Xpert Xpress, 45min) had a PPA of 98%2.
Myself and other colleagues looked more closely at the clinical characteristics of false negative test results on the IDNOW. Overall, we found 82% PPA, and 8 patients with false negative tests. Interestingly, a majority of these patients were tested over 2 weeks after their initial onset of symptoms. The virus is known to be at its highest levels at the beginning of symptom onset. So the test may not be limited, but it should be used in the correct clinical context (< 2weeks from symptom onset). After that time, other RT-PCR based tests are more appropriate.
As clinical laboratorians, we often hear: “the right test for the right patient at the right time.” Now with so many platforms available for use in different contexts, we should help guide clinicians to Choose Wisely.
References
- Harrington A et al. Comparison of Abbott ID Now and Abbott m2000 methods for the detection of SARS-CoV-2 from nasopharyngeal and nasal swabs from symptomatic patients. JCM 2020. PMID: PMID: 32327448
- McDonald et al. Diagnostic Performance of a Rapid Point of Care Test for SARS-CoV-2 in an Urban ED Setting. Academ. Emerg. Med. 2020. PMID: 32492760
- Zhen W et al. Clinical Evaluation of Three Sample-To-Answer Platforms for the Detection of SARS-CoV-2. JCM 2020. PMID: 32332061
- Basu A et al. Performance of the rapid Nucleic Acid Amplification by Abbott ID NOW COVID-19 in nasopharyngeal swabs transported in viral media and dry nasal swabs, in a New York City academic institution. BioRxiv 2020.

-Jeff SoRelle, MD is a Chief Resident of Pathology at the University of Texas Southwestern Medical Center in Dallas, TX. His clinical research interests include understanding how the lab intersects with transgender healthcare and improving genetic variant interpretation.
