Case History
The patient is a 53 year old male with a past medical history of chronic obstructive pulmonary disease, who presented to the emergency department with one day of right calf pain, worse with weight-bearing, with radiating paresthesias, and a pale, cold right foot. He also endorsed a history of intermittent fatigue and knee pain. The patient works on farm and has an 82 pack year smoking history. He was diagnosed with a right popliteal artery occlusion and started on IV heparin. A transthoracic echocardiogram revealed an aortic valve mass.
Five days after admission he underwent a thromboembolectomy of the occluded vessel. A further six days later he underwent a procedure to excise the aortic valve mass, but ended up having an aortic valve replacement. Cardiothoracic surgery described a friable mass with a large base, consistent with a vegetation that might be seen in infective endocarditis, and sent the mass for surgical pathology and aerobic and anaerobic cultures. He was started on empiric vancomycin by infectious disease.
The patient denied recent fevers, chills, sweats, weight loss or changes in appetite, cough, chest pain, abdominal pain, nausea, vomiting, diarrhea, constipation, painful urination, rash, or unusual bone or joint pain. Doxycycline and rifampin were added for further coverage.
Laboratory Identification
Blood cultures drawn on admission showed no growth at 5 days. Initial gram stain of tissue from the mass showed many gram positive beaded rods. Anaerobic cultures of this tissue grew a single colony of Micrococcus and a single colony of a gram positive bacilli, which also grew aerobically and was identified by Mayo as Corynebacterium spp., not jeikeium. Serology for Bartonella was negative. Q fever serology showed elevated titers of phase I Ab IgG only.
Surgical pathology of the aortic valve mass is shown below:
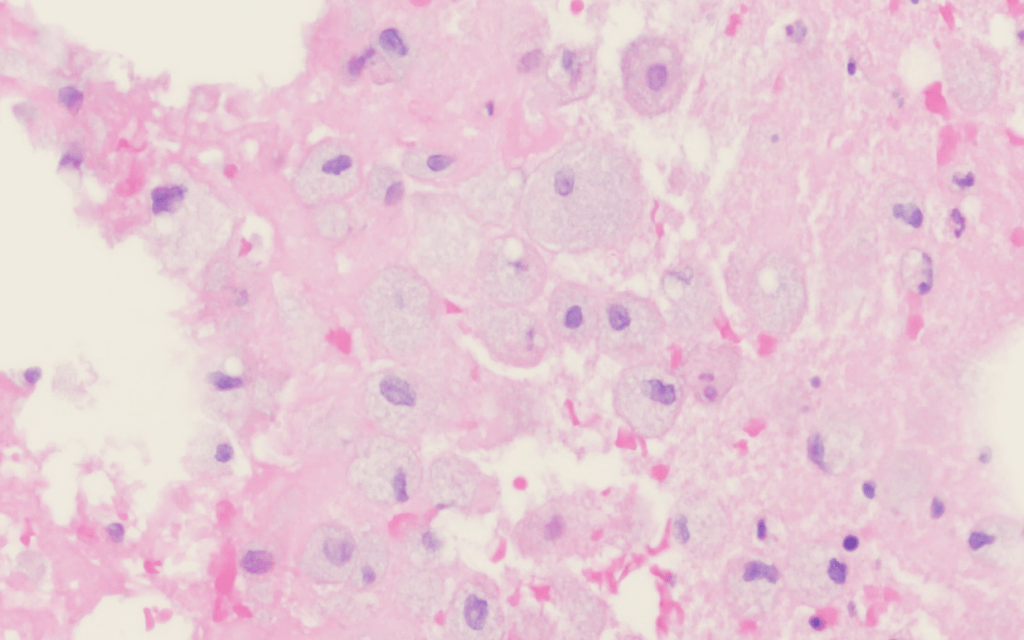
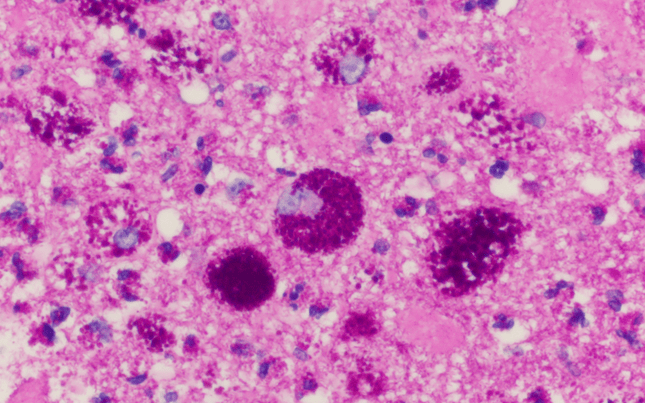
GMS, B&B, AFB, and Fite staining were negative for definitive organisms.
A second set of blood cultures showed no growth and 5 days, and AFB cultures were negative, and second Q fever serology showed a decrease in the titer of phase I Ab IgG.
A PCR of residual heart valve tissue identified Tropheryma whipplei.
Discussion
The diagnosis of Tropheryma whipplei is made by T whipplei PCR, PAS stain, or T whipplei immunohistochemical staining.1 As these are all non-routine tests for a microbiology work-up, the diagnosis depends on high clinical suspicion.
Most often seen in the gut, T whipplei infection classically manifests as arthralgias, abdominal pain, weight loss, and diarrhea.2 However, it is also a rare source of culture-negative endocarditis, as seen in the case above.
The organism is a gram positive bacillus that is common in the environment and found in the saliva of up to 35% of healthy hosts.3 Furthermore, IgG antibodies to T whipplei have been detected in the blood of up to 70% of healthy individuals.4 Microscopically, there is minimal inflammatory response to this organism. Because of this and the classic symptoms, the characteristic foamy macrophages were initially thought to be indicative of a metabolic disorder.5 Once discovered and studied, it was found to most commonly affect males of European descent, which with the minimal inflammatory response to the organism led to the postulation that this population may have a heritable immunodeficiency.6 Others have suggested that the organism itself may have a role in down-regulating the immune response.7 A variety of immunologic disturbances have been associated with the disease, including down-regulation/absence of MHC II molecules and general dysfunction of monocytes/macrophages.1,7,8
Treatment varies by extent of disease, but it generally includes ceftriaxone or penicillin G followed by an extended course of TMP-SMX.1
In the case of our patient, he demonstrated symptomatic improvement after aortic valve repair followed by four weeks of ceftriaxone, with a plan to transition to TMP-SMX for one year.
References
- Apstein, MD, and T Schneider. “Whipple’s Disease.” UpToDate, Wolters Kluwer, 28 June 2019. Accessed 23 March 2020: https://www.uptodate.com/contents/whipples-disease?search=whipples%20disease%20children&source=search_result&selectedTitle=4~70&usage_type=default&display_rank=4#H703772001
- Durand DV, Lecomte C, Cathébras P. “Whipple disease. Clinical review of 52 cases.” Medicine (Baltimore). 1997;76(3):170.
- Street S, Donoghue HD, Neild GH. “Tropheryma whippelii DNA in saliva of healthy people.” Lancet. 1999;354(9185):1178.
- Raoult D, Birg ML, La Scola B, et al. “Cultivation of the bacillus of Whipple’s disease.” N Engl J Med. 2000;342(9):620.
- Whipple GH. “A hitherto undescribed disease characterized anatomically by deposits of fat and fatty acids in the intestinal and mesenteric lymphatic tissues.” Bull. Johns Hopkins Hosp. 1907; 18:382–391.
- Fenollar F, Puéchal X, Raoult D. “Whipple’s Disease.” N Engl J Med. 2007;356(1):55.
- Ectors NL, Geboes KJ, De Vos RM, et al. “Whipple’s disease: a histological, immunocytochemical, and electron microscopic study of the small intestinal epithelium.” J Pathol. 1994;172(1):73.
- Moos V, Schmidt C, Geelhaar A, et al. “Impaired immune functions of monocytes and macrophages in Whipple’s disease.” Gastroenterology. 2010;138(1):210.
-Frederick Eyerer, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.
-Thomas Koster, DO is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.

This one was a doozy
what is your conclusion or recommendation about this case?
Hi Jomailah, thanks for your question. The conclusions that can be drawn from this case are: T whipplei is an unusual organism in regards to its relationship with the host’s immune system, it is a rare cause of culture-negative endocarditis, and diagnosis depends on high clinical suspicion.