Case History
80 year old male patient with history of CLL presented to the emergency room with cough and not feeling well. He was diagnosed with CLL 4 years ago; had been asymptomatic and hence had not received any treatment. CBC done in the emergency room revealed a markedly elevated WBC count of 136 K/uL, decreased hemoglobin of 6.4 g/dl and mildly decreased platelet count at 131 K/uL.
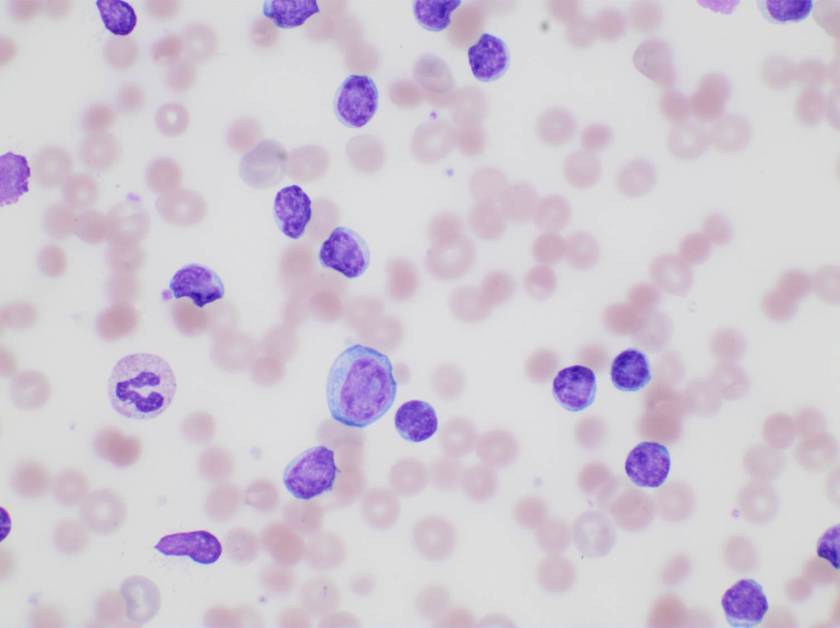
Examination of peripheral blood smear revealed marked lymphocytosis (114.91 K/uL). Majority of the lymphocytes were small with round to oval nuclei. Few larger cells with morphology consistent with prolymphocytes were also noted (overall <5%). Further there was increased polychromasia and spherocytes were easily identified. The patient’s blood type was A positive and the antibody screen was positive. Direct antiglobulin test was positive (IgG) and the antibody identification panel was consistent with the presence of a warm autoantibody. His bilirubin and LDH were both elevated at 3.1 g/dl and 574 U/L, respectively.
The findings were consistent with warm immune mediated hemolysis.
Discussion
Autoimmune hemolytic anemia (AIHA) due to the presence of warm agglutinins is mostly always due to the presence of IgG antibodies that react with protein antigens on the red blood cell (RBC) surface at body temperature.
Underlying causes or conditions that may be associated with AIHA include the following:
- Preceding viral infections (usually in children).
- Typical AIHA due to the presence of warm agglutinins has been described in patients with HIV infection.
- Autoimmune and connective tissue diseases (eg, systemic lupus erythematosus, autoimmune lymphoproliferative syndrome).
- Immune deficiency diseases, such as common variable immunodeficiency.
- Malignancies of the immune system (eg, non-Hodgkin lymphoma, chronic lymphocytic leukemia [CLL], with a higher incidence in those treated with purine analogs).
- Prior allogeneic blood transfusion, hematopoietic cell transplantation, or solid organ transplantation
The incidence of autoimmune hemolytic anemia (AIHA) in patients with CLL is difficult to determine with certainty. As many as one-third of patients with CLL may develop AIHA over the course of their illness unrelated to treatment modality. The prevalence increases with disease stage, from a rate of approximately 4 percent in Binet stage A to 10 percent in stages B and C. The incidence of AIHA may be higher following purine analog treatment.

-Neerja Vajpayee, MD, is the director of Clinical Pathology at Oneida Health Center in Oneida, New York and is actively involved in signing out surgical pathology and cytology cases in a community setting. Previously, she was on the faculty at SUNY Upstate for several years ( 2002-2016) where she was involved in diagnostic work and medical student/resident teaching.
