Case History
Scenario 1: A 51 year old male with a history of diabetes, hypertension, coronary artery disease, gastric ulcer, chronic kidney disease and bilateral below knee amputation presented with epigastric pain, nausea, and vomiting. He was febrile and tachycardic. Computerized scan showed ascending/ transverse colitis and cholelithiasis. Blood cultures grew gram negative rods; the Biofire BCIDv2 panel reported Enterobacter cloacae with no genotypic, resistance markers detected. Phenotypic antimicrobial susceptibility testing (AST) from the Microscan Walkaway revealed resistance to ertapenem (>1mg/ml) but susceptibility to meropenem (£ 1mg/ml). Additionally, the isolate was resistant to 3rd-generation cephalosporins, fluoroquinolones, and intermediate-resistant to tetracyclines. Identification was confirmed by the MALDI-TOF MS upon growth on agar plates. The isolate was subbed with a meropenem disk to select for carbapenem resistance for further confirmatory testing. A Cepheid Carba-R test was ran on a sweep of the isolate growing near the carbapenem disk, which resulted in no carbapenemases detected. Results from E-tests with meropenem and ertapenem were consistent with original phenotypic result. Here, we reported the discrepant phenotypic result and genotypic results as is.
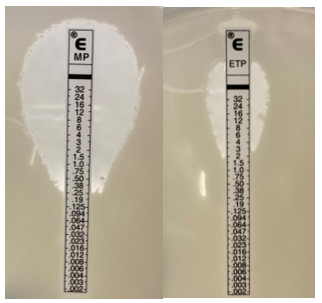
Scenario 2: An 80 year old female underwent a Whipple procedure for a pancreatic mass. A wound culture was submitted from the operating room which grew both Streptococcus anginosus and Enterobacter cloacae complex. Phenotypic AST for the E. cloacae revealed susceptibility to ertapenem (≤0.5 mg/ml) but resistance to meropenem (4 mg/ml). The isolate was pan-susceptible to other drug classes (aside from intrinsic resistance). Similar to Case 1 above, identification was confirmed by the MALDI-TOF MS and the isolate was subcultured with selective pressure. A Cepheid Carba-R test did not detect any carbapenemases. However, upon repeating a phenotypic test, both ertapenem and meropenem were susceptible. Our investigation here led to the avoidance of reporting an incorrect phenotypic AST result.
Discussion
Genotype-to-phenotype discrepancies may occur in antimicrobial susceptibility testing. For example, an antimicrobial resistance (AMR) gene may be detected in a phenotypically susceptible isolate or an AMR gene may not be detected in a phenotypically resistant isolate. Such discordant results should be investigated so appropriate antimicrobial therapy is used on these patients. This leads us to an important question “What can laboratories do to solve these discrepancies?”
The first step in detection of discrepancies requires educating and teaching the lab staff to be vigilant in looking for odd susceptibility patterns (from results within a drug class and also the overall AST profile). Next, check if there was pure isolation of the organism on the purity plate; if not, each individual isolate should be subbed, identified and re-tested on both genotypic and phenotypic platforms. Of note, subbing the bacteria under selective antibiotic pressure (e.g. growing the isolate on agar plate with an antibiotic disk) can increase the potential of detecting resistance. Alternative methods (e.g. CarbaNP, mCIM, etc) could be considered if one is looking into specific resistant mechanisms. Due diligence in checking for clerical, transcription errors and contamination on equipment, especially when there is a consistent pattern of detection for a specific molecular target, is highly recommended. As such, a lab should maintain constant communication with the test manufacturer in case there are issues with batches or lots of reagents.1,2
While these rapid, genotypic panels tend to include the more common AMR mechanisms, there are still other mechanisms of resistance not on the panels. For gram negatives, AMR mechanisms such as AmpC beta-lactamases, porin mutations, efflux pumps and rare carbapenemases such as GES, IMI, and SME types are typically not included.3 Additionally, although the gene blaCTX-M is used as a marker for Extended Spectrum Beta-Lactamases (ESBL), different variants of ESBLs confer different cephalosporin (e.g. 3rd and 4th generation) phenotypes.4 A heteroresistant subpopulation, decreased or lack of expression of an AMR gene may also be potential explanations.
If a discrepancy is not resolved, it is suggested to report the isolate as resistant. If both the discrepant genotypic and phenotypic results are reported, one should consider recommending an infectious diseases consult or to contact the antimicrobial stewardship team.1 Additional information and suggested laboratory workflow can be found in Appendix H of the M100 guidelines from the Clinical Laboratory and Standards Institute.2 While molecular AMR approaches have many advantages such as a shorter turnaround time, phenotypic susceptibility testing can still offer valuable clinical information.5
- CLSI. Performance Standards for Antimicrobial Susceptibility Test. CLSI supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute; 2022, Edition 32
- Yee R, Dien Bard J, Simner PJ. The Genotype-to-Phenotype Dilemma: How Should Laboratories Approach Discordant Susceptibility Results? J Clin Microbiol. 2021 May 19;59(6):e00138-20.
- Tamma PD, Sharara SL, Pana ZD, Amoah J, Fisher SL, Tekle T, Doi Y, Simner PJ. 2019. Molecular epidemiology of ceftriaxone non-susceptible Enterobacterales isolates in an academic medical center in the United States. Open Forum Infect Dis 6:ofz353.
- Paterson DL, Bonomo RA. 2005. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev 18:657–686.
- Dien Bard J, Lee F. 2018. Why can’t we just use PCR? The role of genotypic versus phenotypic testing for antimicrobial resistance testing. Clin Microbiol Newsl 40:87–95. 10.1016/j.clinmicnews.2018.05.003.

–Rami Abdulbaki, MD is a Pathology Resident (PGY-3) at The George Washington University Hospital. His academic interest includes hematopathology and molecular pathology.

-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
