Case History
An 80 year old male from central Vermont with a history of coronary artery disease, hypertension, hyperlipidemia, hypothyroidism, polymyalgia rheumatica, and osteoarthritis status post bilateral knee replacements presented to the ED for fevers, chills, rigors, and fatigue complaining of a home temperature reading of 39.4C (103F). He explained that within the past week he visited a fair to enjoy petting farm animals and trying locally grown produce, meat, and dairy. In the ED he continued to complain of fever, chills, and fatigue, but did not endorse headaches, neck pain, chest pain, SOB, cough, abdominal pain, nausea, vomiting, or diarrhea. An open wound on his left arm was noted. Labs revealed mildly elevated lactic acid, hyponatremia, chronic anemia, but no leukocytosis.
Microbiology
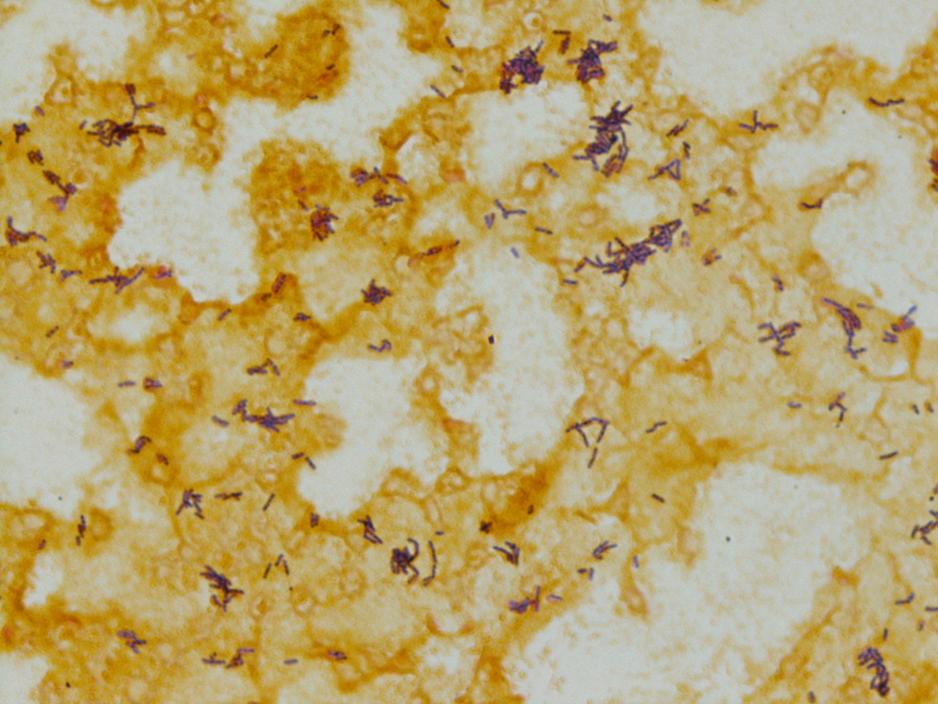
Bacteremia was suspected, and blood cultures obtained. The next day, his blood cultures were positive. Before an extensive workup involving additional cultures and MALDI-TOF, a gram stain was performed and is shown in Image 1. Also, a preparation from a young broth culture demonstrated motility. Both findings indicate Listeria monocytogenes.
Discussion
Listeria monocytogenes is a gram positive rod. Features that aid in its diagnosis include a narrow zone of beta hemolysis, catalase positivity, tumbling motility, and that it is a facultative intracellular organism.
Listeria monocytogenes has one to five peritrichous flagella and demonstrate a “tumbling motility” after incubation of a broth culture at room temperature from 8-24 hours. Listeria monocytogenes also demonstrate a “Christmas tree” or “umbrella” (shown below) pattern of motility when inoculated into a semi solid agar, or “motility medium” (Image 2). This pattern occurs because it grows best in a zone of reduced oxygen tension about 0.5cm below the surface that is also is not strictly anaerobic.1 It also has intracellular motility via polymerization of actin, referred to as “actin rockets,” and can even use this method to spread from one cell to another.

Listeria monocytogenes prefers colder temperatures and is often acquired through consumption of un-pasteurized refrigerated dairy products, deli meats, or produce. Pregnant individuals are more likely to acquire infection as are the young, elderly, or the immunocompromised. Listeria monocytogenes can cause meningitis, usually in newborns or the elderly. Central nervous system or bloodstream infections are treated with ampicillin and gentamycin.2
References
- Allerberger F. Listeria: growth, phenotypic differentiation and molecular microbiology. FEMS Immunol Med Microbiol. 2003 Apr 1;35(3):183-9. doi: 10.1016/S0928-8244(02)00447-9. PMID: 12648835. (n.d.).
- Gelfand, M., Thompson, J., Geeta S. (2021). Treatment and prevention of Listeria monocytogenes infection. UpToDate. Retrieved September 2, 2021, from https://www-uptodate-com.ezproxy.uvm.edu/contents/treatment-and-prevention-of-listeria-monocytogenes-infe. (n.d.).
-Joe Teague is a Pathology Student Fellow and Brianna Waller, MD is a 3rd year Anatomic and Clinical Pathology Resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
