Case History
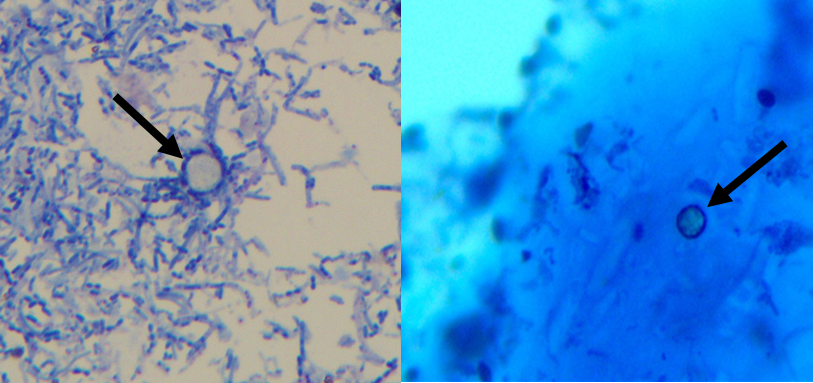
A woman in her 40s presented to her primary care physician in summer 2020 with mild abdominal pain, diarrhea, nausea, and headache. She experienced loose bowel movements 3 – 4 times per day for the past 18 days. She denied bloody stools, travel, consumption of raw or undercooked meats or unpasteurized dairy, contact with animals, or recent antibiotic use. SARS-CoV-2 PCR was negative. A stool sample was collected and sent for an enteric panel PCR (Salmonella, Shigella, Campylobacter, and Shiga toxin), a bacterial stool culture (Aeromonas, Plesiomonas, and Vibrio), and an ova and parasite (O&P) exam with a request to perform a modified acid-fast stain. While the enteric panel and bacterial stool culture were negative, the following organism was observed on the modified acid-fast stain (Image 1). This organism measured approximately 9 µm, was variably modified acid-fast, and had a wrinkled-cellophane appearance. The organism was identified as a Cyclospora cayetanensis oocyst. The patient later shared that she had consumed a bagged salad mix that was implicated in the ongoing Cyclospora outbreak.
Cyclospora cayetanensis
Cyclospora cayetanensis, a coccidian protozoan, is transmitted through ingestion of food or water contaminated with infectious oocysts. While infected humans shed oocysts in their stool, these oocysts are unsporulated and non-infectious at the time of excretion. In order to sporulate and become infectious, these excreted oocysts must incubate in the environment for 7 – 15 days post-excretion. Due to the required incubation post-excretion, direct fecal-oral transmission cannot occur.
Endemic areas include Central and South America, Middle East, South East Asia, and the Indian subcontinent. In non-endemic areas, travelers make up a large proportion of cases. Local outbreaks in non-endemic areas are often due to contaminated food sources. Most commonly the source of these outbreaks arise from consumption of raw fruits and vegetables that are difficult to thoroughly clean. These include leafy green vegetables (salad mixes, lettuce), herbs (basil, cilantro), and raspberries. Moreover, Cyclospora is resistant to many disinfectants used in the food industry. As exposure to this parasite is through contaminated food and water, infected patients are also at risk for other food and waterborne parasites including Cryptosporidium.
Once infectious oocysts are ingested, symptoms are typically observed after a one week incubation. Clinical presentation of Cyclospora infection includes diarrhea, nausea, fatigue, low grade fever, and weight loss. Although Cyclospora causes infections in both immunocompromised and immunocompetent individuals, symptoms may be severe and prolonged in immunocompromised patients, particularly in HIV and AIDS patients. Children and elderly individuals are also at higher risk for severe disease. Trimethoprim-sulfamethoxazole is the standard treatment. If untreated, symptoms can last for 10 – 12 weeks and may exhibit a relapsing pattern.
Stool samples should be submitted to the clinical microbiology laboratory for microscopic and/or molecular studies. To increase recovery of the organism during intermittent or low burden shedding, multiple stool specimens should be submitted over 2 -3 days. When viewed under a UV fluorescent microscope, Cyclospora oocysts autofluoresce and appear blue or green. While safranin-based stains or UV fluorescent microscopic examination can be used, modified acid-fast staining is commonly performed for the microscopic identification of Cyclospora. Cyclospora oocysts are modified acid-fast variable and measure 8 – 10 µm in diameter, unlike Cryptosporidium oocysts which are modified acid-fast positive and measure 4 – 6 µm in diameter. It is important to alert the clinical microbiology lab if suspecting Cyclospora as stains used in routine O&P exam, including trichrome stains, are not effective in highlighting Cyclospora. Although lab developed tests and FDA cleared multiplex gastrointestinal pathogen panels including Cyclospora are available, molecular assays are not yet routinely used for identification of Cyclospora due limited widespread availability.
References
- Almeria S, Cinar HN, Dubey JP. Cyclospora cayetanensis and Cyclosporiasis: An Update. Microorganisms. 2019;7(9):317. Published 2019 Sep 4. doi:10.3390/microorganisms7090317
- Hadjilouka A, Tsaltas D. Cyclospora Cayetanensis-Major Outbreaks from Ready to Eat Fresh Fruits and Vegetables. Foods. 2020;9(11):1703. Published 2020 Nov 20. doi:10.3390/foods9111703
- Ortega YR, Sanchez R. Update on Cyclospora cayetanensis, a food-borne and waterborne parasite. Clin Microbiol Rev. 2010;23(1):218-234. doi:10.1128/CMR.00026-09
- Garcia LS. Diagnostic Medical Parasitology. 6th Edition. 2016.
- Casillas SM, Bennett C, Straily A. Notes from the Field: Multiple Cyclosporiasis Outbreaks — United States, 2018. MMWR Morb Mortal Wkly Rep 2018;67:1101–1102. DOI: http://dx.doi.org/10.15585/mmwr.mm6739a6

Paige M.K. Larkin, PhD, D(ABMM), M(ASCP)CM is the Director of Molecular Microbiology and Associate Director of Clinical Microbiology at NorthShore University HealthSystem in Evanston, IL. Her interests include mycology, mycobacteriology, point-of-care testing, and molecular diagnostics, especially next generation sequencing.
