I’ve witnessed that radiologists are often hesitant to perform a core biopsy on a spleen due to its vascularity, so when I attend spleen FNAs, I rarely push. Even when the oncology team requests both a core biopsy and FNA for a hematology workup, I will acquire as many passes as possible from an FNA to work up cytomorphology and flow cytometry before risking a core-induced hemorrhagic complication. When I was called to attend an ultrasound-guided spleen biopsy, I went in knowing two things: the patient has both splenic and brain lesions, and I was going to make the most of what I was given. When I arrived in ultrasound, the radiologist informed me that the patient had polycythemia vera (PV), which would explain the splenomegaly, but not the brain lesions. The patient, a 65 year old male, received the diagnosis in 2009 and was managed with phlebotomies for six years until a rising platelet and white blood cell count required an intervention of hydroxyurea. Within 18 months, the patient developed a PE and dizziness and began therapeutic anticoagulation. At the same time, the patient’s “metastatic lesions” were identified on imaging. The first state of business is finding out if his PV had progressed into myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML). There was something… off… about this case though. It didn’t feel like a heme case (not that I prefer non-heme cases… well, okay, I’m a cytotech, so I kind of do). The brain lesions concerned me, and I didn’t know what to infer.
Let’s progress to the FNA. Here are the air-dried, Diff-Quik smears that changed everything.
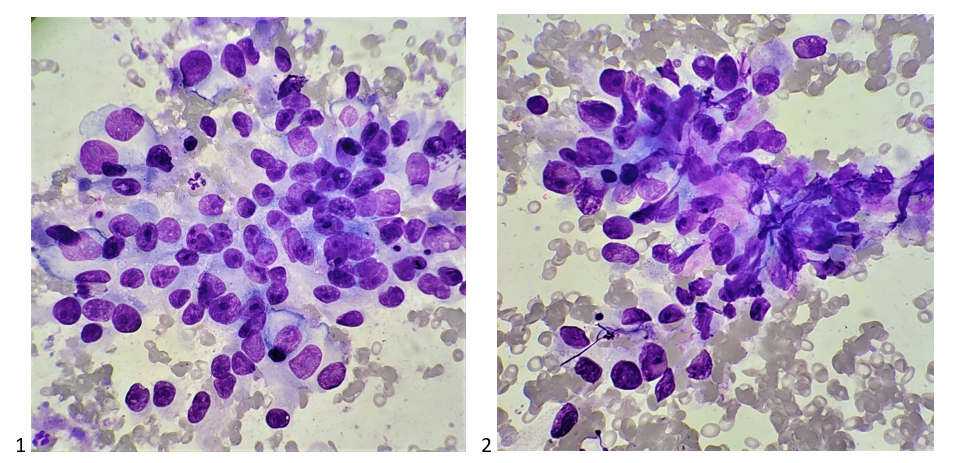
What non-heme surprise is THIS?! Are these histiocytes? There’s no way, those nucleoli are aggressive! Look at the chromocenters! The variation in nuclear size! What epithelial beauty is this? Is it epithelial?! Is that a fibrovascular core? It can’t be sarcomatoid, could it? Twenty inner monologue questions later, “okay, it’s adequate,” I said to the radiologist. But wait… should I do it? Should I press for a core biopsy? The radiologist asked me if I needed anything else for the diagnosis. Perhaps she saw my puzzled expression, compelling her to tell me that she felt the imaging looked weird – she thought it wasn’t a heme case either. At least I’m not alone here. I took a deep breath, expecting the worst and hoping for the best, and I asked the radiologist to collect a core biopsy. She checked the ultrasound Doppler for excessive vascularity, and much to my surprise, she agreed to perform the core. After collecting more FNAs for my cell block and dropping the core biopsies off in surgical pathology, I showed the case to my attending pathologist. He also agreed that we don’t need to triage it for heme. He asked if the patient had any significant history other than PV, splenic lesions, and brain mets, and I told him nothing was reported in his chart. I checked the chart again for good measure while he was running through his differential diagnoses of lung, GI, prostate, etc., and saw the patient was scheduled to see dermatology later that week. I mentioned to that to my attending, and he suggested it could be a melanoma.
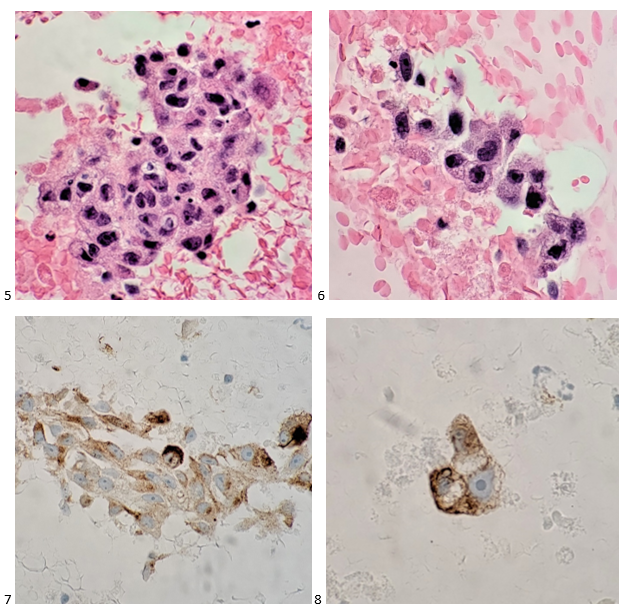
The following morning, I examined the pap-stained slide and began to second guess myself. Was I wrong? Could it be a heme case? Hodgkin’s wasn’t in the differential, and these cells look so much more aggressive than Reed-Sternberg cells. At least we have a core biopsy either way. We could run immunos on the cell block and save the cores for molecular. I screened the pap-stained slides a little longer, focusing on the macronucleoli, the owl-eye and eccentric nuclei, the poorly-differentiated nature of this… MELANOMA. YES! So, the cells might not contain any melanin pigment, but my attending’s inkling was exactly right. Waiting for my cell block to arrive, I listed melanoma as my primary diagnosis with a differential of lung or prostate cancer.

The cell block confirmed my non-heme diagnosis and kept my differentials at bay. The attending pathologist ordered an immunohistochemistry profile of S100, HMB-45, and Melan A, as well as AE1/AE3. The first three immunostains (prior to our adoption of SOX-10) confirmed a diagnosis of metastatic malignant melanoma. Soon thereafter, the patient’s primary lesion was identified on his back, and he was treated with radiation and immunotherapy. Unfortunately, the metastases were not responding to the immunotherapy, and a few days after a clinical trial was offered, the patient passed away.
Melanoma is known as the great mimicker, especially in amelanotic form, and it should always be in the back of your mind as a differential diagnosis. Lack of melanin pigment and a large cherry red macronucleoli leads us to favor lung, prostate, or serous adenocarcinoma), renal cell carcinoma, hepatocellular carcinoma, Hodgkin’s lymphoma, or even an epithelioid sarcoma. This case highlights the need to remember that metastatic melanoma is always a possibility, even when you do not have a primary site or previous clinical history of the disease.

-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
