Clinical History
A 70 year old patient with a history of sarcoidosis, diabetes mellitus type 2, and interstitial lung disease on prednisone presented to an outside hospital with subacute altered mental status and dizziness. Head imaging showed 3 ring-enhancing lesions most concerning for intracranial abscesses and the patient was transferred to a larger institution for management. Upon further imaging and physical examination, 3 additional lesions were found, one in the abdominal wall and two subcutaneous lesions on the extremities. An IR-guided biopsy of the abdominal wall lesion was performed and the specimen was sent for bacterial culture and smear.
Laboratory findings
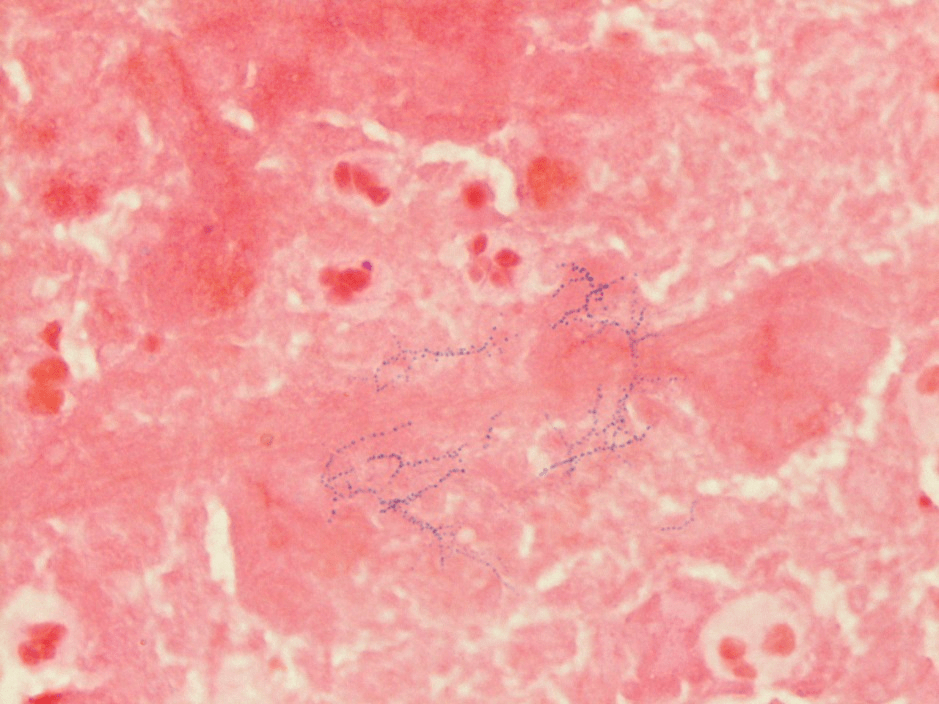
An initial gram stain was interpreted as many neutrophils and no bacteria seen; however, Acridine Orange staining demonstrated the presence of fungi or bacteria on the smear. Further review of the gram stain showed many neutrophils with few filamentous beading and branching gram positive bacilli predominantly in the thick regions of the smear (image 1).
Discussion
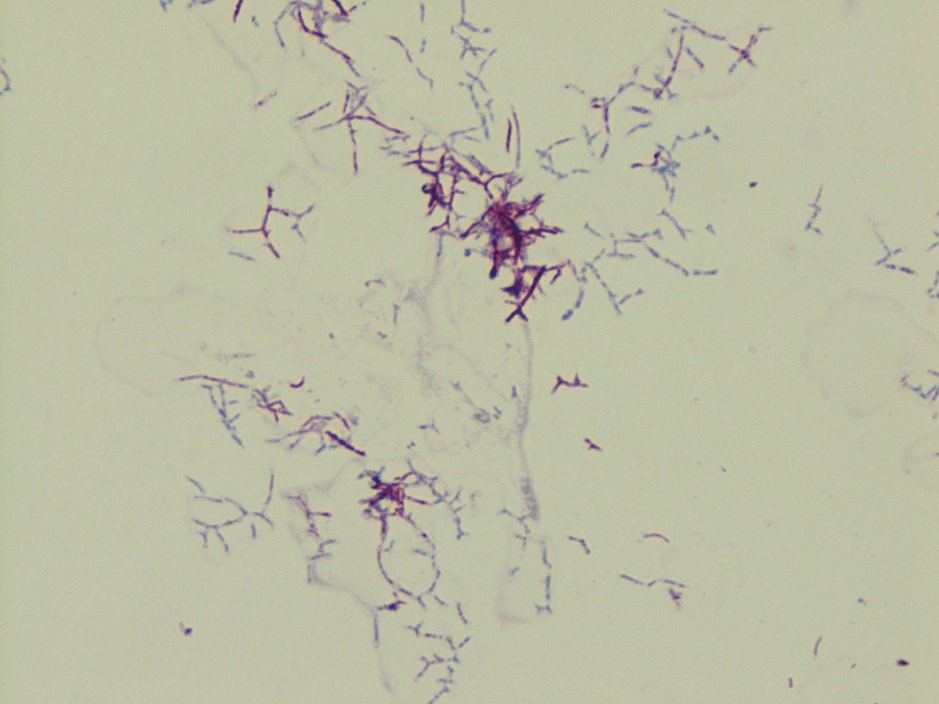
Nocardia encompasses a group of delicate aerobic gram positive and weakly acid fast positive rod-shaped bacteria that, due to their branching appearance, were once thought to be fungi. The N. farcinica species are not found in normal flora, but instead in soil around the world and are most often associated with decaying vegetation. It is the bacteria’s ability to become airborne on dust particles that may result in inhalation and lead to the most common presentation, pulmonary nocardiosis. Other modes of entry include ingestion and cutaneous disease after traumatic inoculation. CNS involvement is a common site for secondary infection.1
The pathogenicity of Nocardia is the result of several mechanisms that the bacteria possess to evade the host’s defense system. Nocardia are often resistant to phagocytosis when they are in their log-phase. If the bacteria are phagocytosed, some species have the ability to inhibit the lysosome-phagosome fusion. Nocardia farcinica, in particular, is especially important to identify as it is more likely to progress to disseminated disease and has a higher rate of antimicrobial resistance.2
Most cases of nocardiosis, as with ours above, are in immunocompromised patients either by disease states such as HIV, diabetes, and malignancy or iatrogenically with corticosteroids or other immunosuppressing or immunomodulating drugs. The clinical presentation of nocardiosis is non-specific and is dependent on the site of infection, but the diagnosis should be on the differential for immunocompromised patients with a suspected CNS abscess, particularly if they have concurrent cutaneous, soft tissue, or pulmonary infections.3
Therapy is based on site of infection and species of nocardia isolated; however, trimethoprim-sulfamethoxazole is accepted as part of the first-line treatment. Severe disease, such as that exhibited in our patient, warrants combination therapy and may include a carbapenem, third generation cephalosporin, or an extended spectrum fluoroquinolone.4 Our patient was originally treated with trimethoprim-sulfamethoxazole and imipenem, but the trimethoprim-sulfamethoxazole was discontinued due to hyperkalemia and the patient was started on Linezolid.
References
- Spelman, Denis. “Microbiology, epidemiology, and pathogenesis of nocardia”. UpToDate, Wolters Kluwer, May 08, 2019. https://www.uptodate.com/contents/microbiology-epidemiology-and-pathogenesis-of-nocardiosis?search=nocardiosis&source=search_result&selectedTitle=3%7E94&usage_type=default&display_rank=3. Accessed on March 10, 2020.
- Bell M, McNeil MM, and Brown JM. Nocardia species (Nocardiosis). 2014. http://www.antimicrobe.org/b117.asp. Accessed on March 24, 2020.
- Spelman, Denis. “Clinical manifestations and diagnosis of nocardiosis”. UpToDate, Wolters Kluwer, May 08, 2019. https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-nocardiosis?search=nocardiosis&source=search_result&selectedTitle=1~94&usage_type=default&display_rank=1. Accessed on March 10, 2020.
- Spelman, Denis. “Treatment of nocardiosis”. UpToDate, Wolters Kluwer, November 11, 2019. https://www.uptodate.com/contents/treatment-of-nocardiosis?search=nocardiosis&source=search_result&selectedTitle=2~94&usage_type=default&display_rank=2. Accessed on March 24, 2020.
-Kayla Elliott, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
