Clinical History
The patient is a 57 year old male with a history of traumatic brain injury in 2005 resulting in quadriplegia and subsequent neurogenic bladder with chronic spasms. In 2016 the patient underwent cystoprostatectomy, proctectomy, and ureteroenteric anastomosis to colon. The post-operative period was complicated by the formation of a presacral abscess consisting of MSSA and E. coli. Drain placement failed to resolve the abscess and drain studies showed the formation of a fistula to the patient’s rectal stump. The subsequent 3-year period consisted of repeat drain placements and laparotomy to drain and wash out multiple small collections of fluid seen on imaging. Bacterial cultures during this interval grew mixed gram positive and gram negative enteric bacteria, treated primarily with ertapenem. In January of 2020, the patient underwent exploratory laparotomy with debridement and drainage of pelvic abscess. Tissue cultures from the procedure grew MRSA and vancomycin was prescribed for treatment. Vancomycin was switched to daptomycin for more favorable dosing and ertapenem was added to his treatment plan. Four weeks after his operation, the patient reported pain at his drain site and the fluid in his Jackson-Pratt (JP) drain had turned green. Fluid from the JP drain was submitted for microbiological work-up.
Laboratory Findings
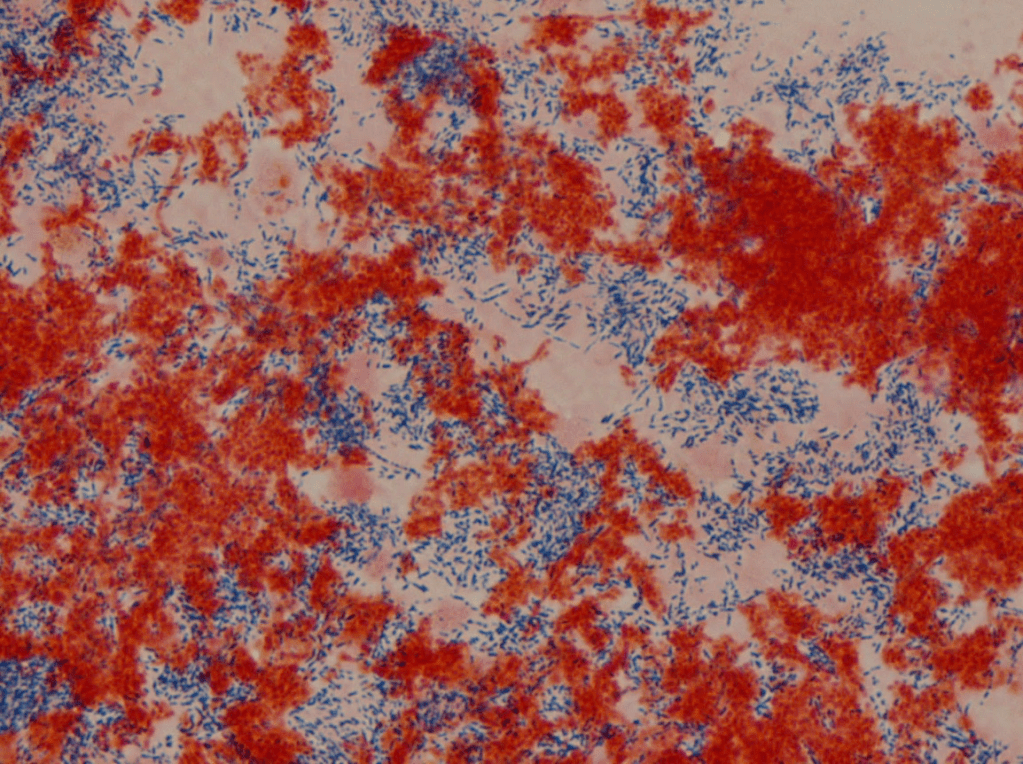
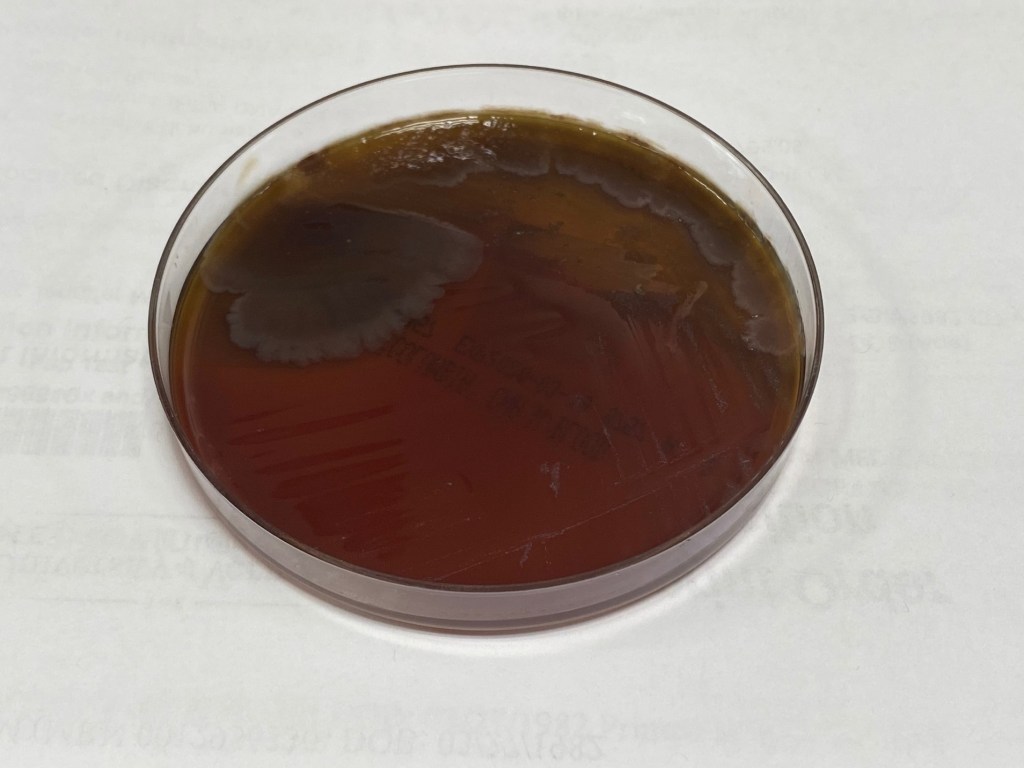
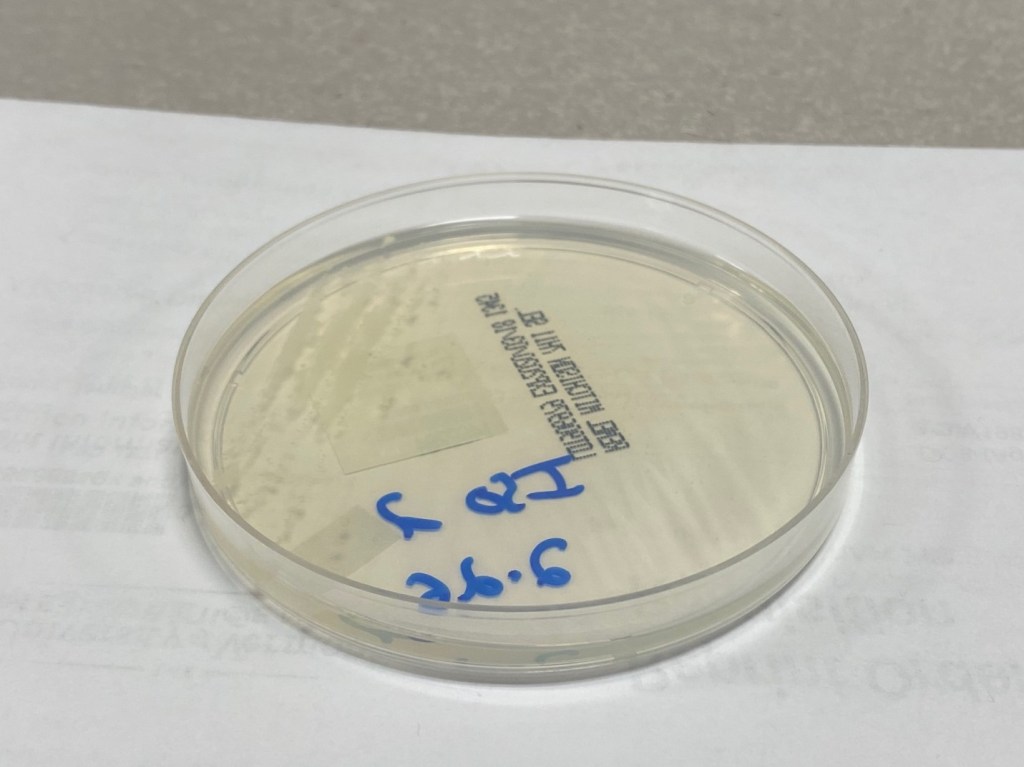
Gram stain of the fluid from the JP drain showed neutrophils, many gram negative bacilli, and beaded gram-positive bacilli. Modified Kinyuon testing was positive for acid-fast bacilli (AFB) and cultures were ordered for mycobacteria as well as Nocardia. The gram negative bacilli was isolated and identified as Pseudomonas aeruginosa by MALDI-ToF. The beaded gram-positive bacilli were isolated on CNA agar and identified by MALDI as Mycobacterium chelonae. Concordant morphology was observed on mycobacterial culture. Nocardia culture was overgrown by P. aeruginosa.
Discussion
Rapidly growing mycobacteria (RGM) include the three most common clinically relevant species: Mycobacterium abscessus, Mycobacterium fortuitum, and Mycobacterium chelonae.
The RGM are environmental organisms found worldwide that usually grow in subculture within one week (eg, rapidly, as compared with other mycobacteria). M. abscessus is the most commonly encountered species of this group isolated from clinical respiratory specimens, M. fortuitum is the most common from non-respiratory specimens, and M. chelonae primarily impacts immunosuppressed patients and may also cause surgical wound infections.
Postoperative infections with RGM have occurred following various procedures including cosmetic surgery procedures, augmentation mammoplasty, laser in situ keratomileusis (LASIK), and heart surgery.1-8 Infection is characterized by multiple recurrent abscesses around the surgical wound.
Diagnosis for non-pulmonary disease is made by culture of the specific pathogen from drainage material or biopsy of the affected site. The isolation of organisms from sterile, closed sites, such as bone marrow or blood or from a skin biopsy (in the setting of multiple lesions), is diagnostic of the disease. Once an isolate has been identified as a nontuberculous mycobacteria (NTM), the species should be identified. However, identification of RGM in most laboratories is either incomplete or imprecise. M. abscessus isolates are frequently identified simply as “M. chelonae/abscessus complex,” or if they are specifically identified as “M. abscessus,” they are not accurately sub-speciated.
Susceptibility testing should be performed against a number of antibacterial agents, however, there is no established minimum inhibitory concentration (MIC) cutoff for susceptibility or resistance. M. chelonae is typically treated with Macrolide antibiotics, particularly azithromycin and clarithromycin. M. fortuitum, M. abscessus, and M. chelonae are resistant to the antituberculosis agents rifampin, ethambutol, and isoniazid, so susceptibility testing of RGM should not be performed with these.
The clinicians in our case suspected that the M. chelonae culture from the patient’s JP drain was most likely a contaminant as the same organism was never isolated from previous tissue or fluid cultures. He was continued on daptomycin, ertapenem, and ciprofloxacin was added to cover P. aeruginosa. The patient responded well with resolution of his localized symptoms at the site of the JP drain. Unfortunately, he continues to suffer from multiple, recurring presacral abscesses.
References
- Rimmer J, Hamilton S, Gault D. Recurrent mycobacterial breast abscesses complicating reconstruction. Br J Plast Surg 2004; 57:676.
- John T, Velotta E. Nontuberculous (atypical) mycobacterial keratitis after LASIK: current status and clinical implications. Cornea 2005; 24:245.
- Freitas D, Alvarenga L, Sampaio J, et al. An outbreak of Mycobacterium chelonae infection after LASIK. Ophthalmology 2003; 110:276.
- Sampaio JL, Junior DN, de Freitas D, et al. An outbreak of keratitis caused by Mycobacterium immunogenum. J Clin Microbiol 2006; 44:3201.
- Edens C, Liebich L, Halpin AL, et al. Mycobacterium chelonae Eye Infections Associated with Humidifier Use in an Outpatient LASIK Clinic–Ohio, 2015. MMWR Morb Mortal Wkly Rep 2015; 64:1177.
- Toy BR, Frank PJ. Outbreak of Mycobacterium abscessus infection after soft tissue augmentation. Dermatol Surg 2003; 29:971.
- Centers for Disease Control and Prevention (CDC). Mycobacterium chelonae infections associated with face lifts–New Jersey, 2002-2003. MMWR Morb Mortal Wkly Rep 2004; 53:192.
- Wallace RJ Jr, Brown BA, Onyi GO. Skin, soft tissue, and bone infections due to Mycobacterium chelonae chelonae: importance of prior corticosteroid therapy, frequency of disseminated infections, and resistance to oral antimicrobials other than clarithromycin. J Infect Dis 1992; 166:405.
- Wallace RJ Jr, Brown BA, Onyi GO. Susceptibilities of Mycobacterium fortuitum biovar. fortuitum and the two subgroups of Mycobacterium chelonae to imipenem, cefmetazole, cefoxitin, and amoxicillin-clavulanic acid. Antimicrob Agents Chemother 1991; 35:773.
-Will Humphery, MD is a 1st year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
