Case History
The patient is a 31 year old man with a history of intravenous drug use with last reported use nine months previous, who reports low back pain. The patient’s symptoms started as a mild pain and progressively worsened over two weeks to the point that he was unable to stand or ambulate. He also developed intermittent radiation of pain to the bilateral lower extremities and associated symptoms of chills and diaphoresis. Blood cultures were sent. MRI showed an epidural abscess at the level of L5-S1. The patient underwent lumbar spinal decompression surgery, and intra-operative cultures were sent for evaluation.
Laboratory Identification
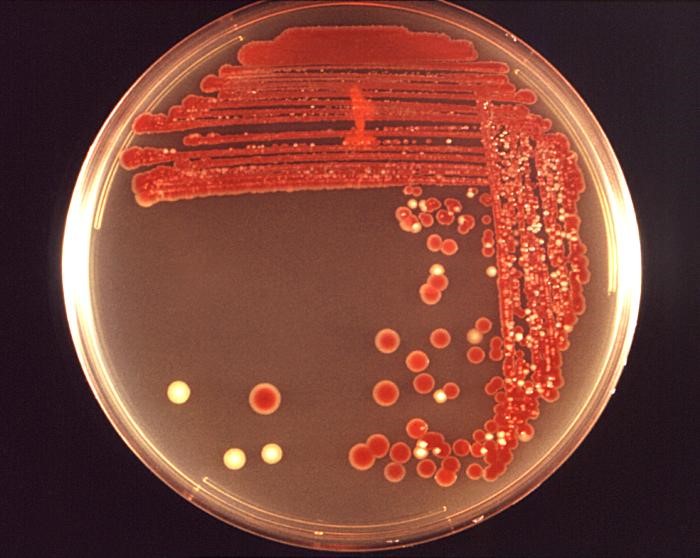
Gram smear of blood cultures showed gram negative bacilli (Image 1). Culture of the abscess specimen and blood cultures showed growth on chocolate, blood, and MacConkey agar; growth on MacConkey plates did not show lactose fermentation (Image 2,3). MALDI-TOF identified this organism as Serratia marcescens.



Discussion
Serratia marcescens is a motile, facultatively anaerobic, gram negative bacillus of the Enterobacteriaciae family. Some strains of Serratia produce a distinctive brick red pigment, prodigiosin (Image 4), although non pigmented strains are frequently isolated from human infection sites. Serratia marcescens is one of the few Enterobacteriacea that produces DNAse, lipase, and gelatinase. It does not usually ferment lactose. This species is widely present in the environment, including in animals, insects, plants, water, and soil, but unlike other Enterobacteriaciae species it is not a typical component of normal human fecal flora.
Eight species of Serratia have been found to cause infections in humans. Of these, >90% are caused by Serratia marcescens (1). This is a rare cause of infection in immunocompetent hosts but can cause opportunistic nosocomial infections, especially following invasive procedures such as such as intravenous catheterization, respiratory intubation, and urinary tract manipulations. The most common infections caused by Serratia marcescens are urinary tract infections, pneumonia,surgical wound infections, eye infections, and bacteremia. Multiple hospital outbreaks of Serratia have been reported, with sources of infection including tap water, soap, blood transfusion products, and injected medications (2). It has also been described as a cause of endocarditis in injection drug users (3).
Serratia is intrinsically resistant to ampicillin, ampicillin-sulbactam, and 1st and 2nd generation cephalosporins due to an inducible, chromosomal AmpC beta-lactamase. Resistance to later-generation cephalosporins may be induced through exposure to these antibiotics, despite not being detected on initial antibiotic susceptibility tests. Thus, susceptibility testing is misleading and thirdgeneration cephalosporins (such as ceftazidime, ceftriaxone, and cefpodoxime) should be avoided for the treatment of Serratia species regardless of in vitro susceptibility.
References
- Laupland KB, Parkins MD, Gregson DB, Church DL, Ross T, Pitout JD. Population-based laboratory surveillance for Serratia species isolates in a large Canadian health region. Eur J Clin Microbiol Infect Dis. 2008; 27: 89–95.
- Mahlen SD. Serratia infections: from military experiments to current practice. Clin Microbiol Rev. 2011; 24:755.
- Mills J., Drew D. Serratia marcescens endocarditis: a regional illness associated with intravenous drug abuse. Ann Intern Med. 1976; 84:29–35.
-Erica Worswick is a pathology student fellow at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
