Case History
A 44 year old male presented to the emergency department with severe, throbbing back pain in his mid-thoracic spine. He states the pain began a couple weeks ago and noted no recent fevers or night sweats, but does admit to chills. His past medical history is significant for end stage renal disease requiring dialysis, insulin dependent diabetes mellitus, and multiple amputations. On physical examination, there was tenderness to palpation along spine in mid-thoracic region. Lab work showed a normal white blood cell count, C reactive protein of 0.90 mg/dL (0.00 – 0.50 mg/dL), and an erythrocyte sedimentation rate of 60.0 mm/hr (0.0 -10.0 mm/hr). MRI of the spine was consistent with discitis and osteomyelitis at T7-8 with compression fractures causing spinal stenosis and cord compression. Given the concern for an infection process, blood cultures were collected and interventional radiology performed a bone biopsy. The specimen was sent for bacterial, fungal, and AFB cultures as well as for histology.
Laboratory Identification

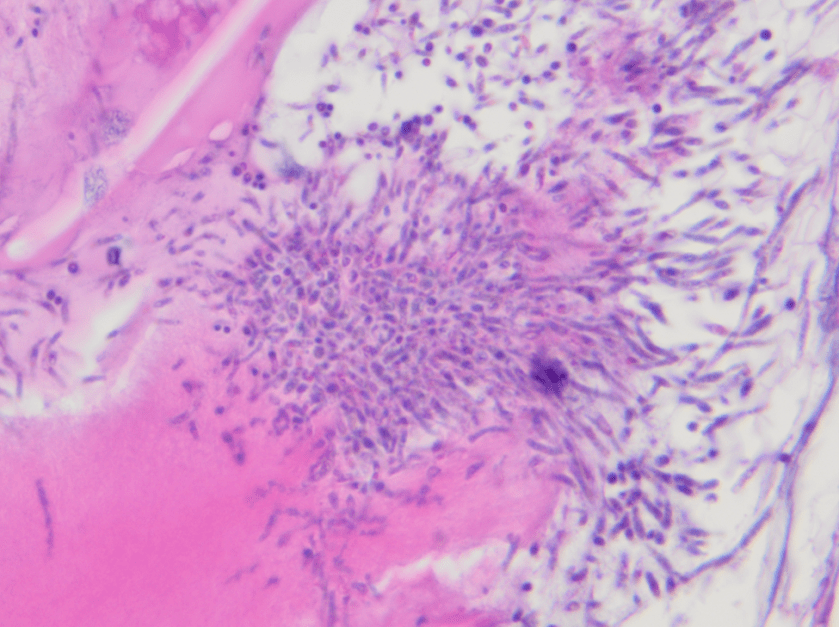
The organism grew as discrete, creamy colonies growing on blood agar and Sabouraud dextrose agar after 48 hours of incubation at 35°C and resembled a yeast. MALDI-TOF mass spectrometry identified the isolate as Candida parapsilosis. Similarly, the surgical pathology specimen showed necrotic bone with inflammation and yeast forms and pseudohyphae consistent with a Candida spp. infection. Blood cultures were negative. On chart review from an outside hospital, it was discovered the patient had an episode of candidemia ten months ago which was thought to be related to his dialysis port.
Discussion
Yeasts are ubiquitous in the environment and make up the normal microbiota of human skin as well as the oral cavity, gastrointestinal tract and genitourinary tract. In general, when Candida spp. cause infections it is thought to an opportunistic infection acquired endogenously and due to exposure to prolonged antibiotics, suppressed immune system, or as a result of intravascular catheters. Those with diabetes mellitus, mucositis, bowel perforations, and intravenous drug users are most susceptible. Infections with Candida parapsilosis are becoming more common, and have the potential to cause invasive disease, such as fungal endocarditis and severe infections in the neonatal population.
In the microbiology laboratory, C. parapsilosis grows rapidly as discrete, creamy colonies on a variety of agars. On cornmeal-Tween 80 agar, C. parapsilosis grows as short, curved pseudohyphae with blastoconidia arranged singly or in small clusters at points of constriction. The arrangement is sometimes described as resembling a sage bush. C. parapsilosis is germ tube negative and is negative for urease. In many laboratories currently, identification is achieved by automated methods, such as Vitek 2, or mass spectrometry, allowing for more rapid and accurate identification.
Anti-fungals, such as echinocandins, azoles, and amphotericin B, are all potential therapeutic options to treat C. parapsilosis infections. CLSI C.parapsilosis specific breakpoints exist for fluconazole, voriconazole,micafungin, caspofungin, and anidulafungin in the M27-S4. Susceptibility testing should be performed on significant isolates from normally sterile sites.
In the case of our patient, infectious disease was consulted and he was started on IV micafungin and then transitioned to oral fluconazole. He had a transesophgeal echo and eye exam performed to ensure he didn’t have endocarditis or an invasive eye infection due to hematogenous spread of the yeast. He was discharged home on long term oral fluconazole.

-Rim Alkawas, MD, is a second year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
