Case History
The patient is a 64 year old male with a history of diabetes mellitus and hypertension who presented as a transfer from an outside hospital with a 2 week history of chest pain and pressure, as well as recurrent fevers, rigors, and soaking sweats, and an echocardiogram concerning for a pericardial effusion. He was also found to have markedly elevated CRP, and mildly elevated troponins, was diagnosed with pericarditis, and was started on colchicine. He continued to have fevers, and developed diarrhea and was transferred for elevation of care. C. difficile PCR was negative, and since the onset of diarrhea coincided with the initiation of colchicine, that was determined to be the cause. Blood cultures on arrival grew a Gram positive rod and a transesophageal echocardiogram was done which again showed pericardial thickening with small effusion, and fluid with fibrinous appearance. There was no evidence of valvular vegetation. At this point the patient was started on IV meropenam as he is allergic to penicillin’s and sulfa drugs. The pericarditis seemed to improve with colchicine so a non-infectious process was favored and a repeat ANA was recommended when he has recovered from his current infection.
Laboratory Identification
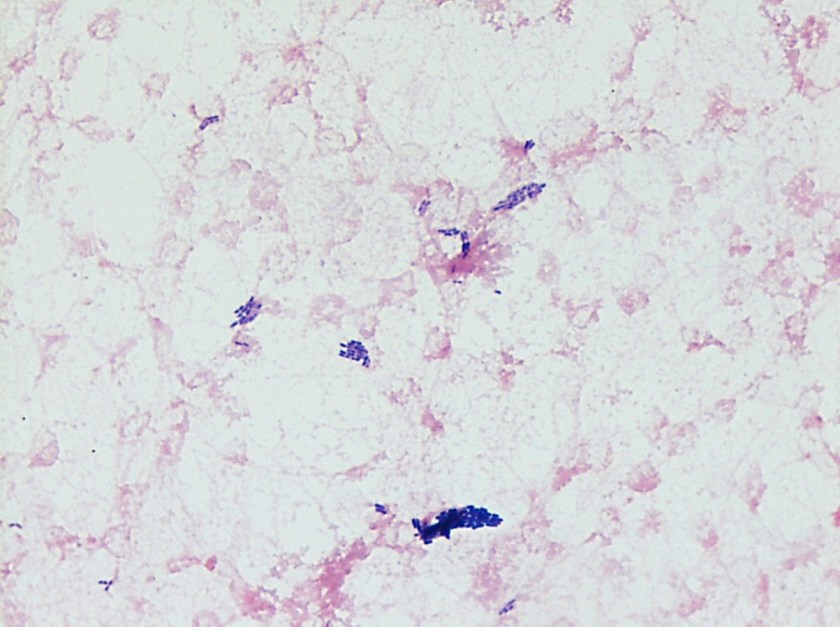
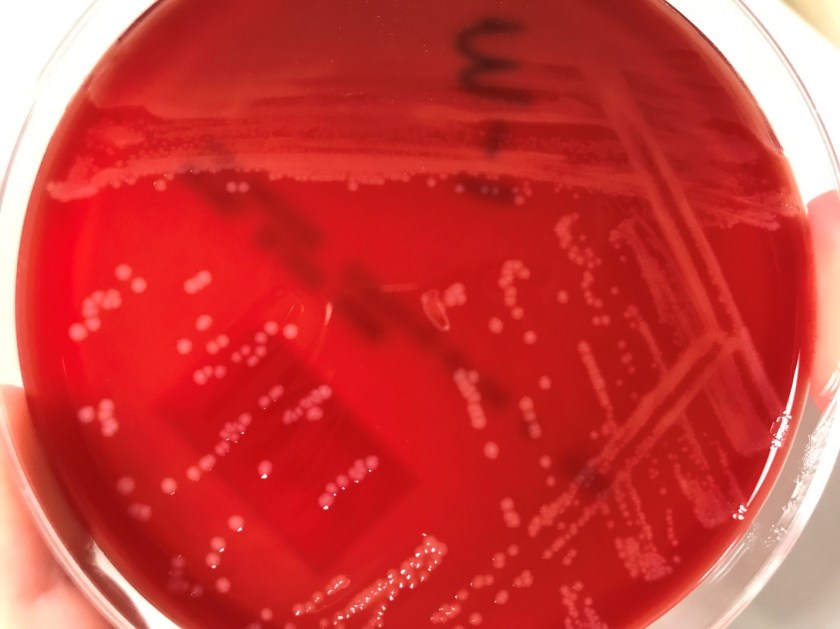
Blood cultures grew grey-white colonies that are gram positive, catalase positive rods with soft beta-hemolysis on the blood agar plate, and tumbling motility under light microscopy. CAMP testing would be positive with Staphylococcus aureus. This was identified as Listeria monocytogenes by the MALDI.
Discussion
Listeria monocytogenes is a gram positive rod that can be found in the soil, water, sewage, vegetation, and as part of the fecal flora of animals. It is facultative intracellular pathogen that is able to invade and survive in human cells including macrophages (1). They possess a surface protein called internalin that interacts with E-cadherin on human cells resulting in endocytosis (1). Once within the cell the bacteria can produce listeriolysin O and other phospholipases which allow it to escape from the phagosome before it fuses with the lysosome, which prevents intracellular killing of the bacteria (2). L. monocytogenes is a common contaminant of food products as it can form biofilms on the food surfaces. Listeria also has the ability to grow a 4°C so it can continue to grow on refrigerated foods (1). Foods such as raw milk, raw vegetables, fish, poultry, and fresh and processed meats are the highest risk for contamination.
Ingestion during pregnancy can result in a flu like illness, occasionally with vaginal discharge, diarrhea, and urinary tract symptoms (1). Infection during pregnancy is particularly dangerous as occult bacteremia with transplacental transmission may occur (2). Infection in utero may result in premature labor and birth of an infected or stillborn fetus. Prognosis is highly dependent on the gestational age at infection.
Non- pregnant adults can also become infected by Listeria. The most common results of ingestion of contaminated food in immunocompetent patients is a transient asymptomatic carrier state, and can be excreted in the feces. Less commonly, febrile gastroenteritis can occur. Immunocompromised patients or those with underlying malignancy tend to present with acute sepsis, meningitis, or meningoencephalitis. Focal infections such as cutaneous infection, abscesses, arthritis, peritonitis, liver/splenic abscess, cholecystitis, artificial joint/graft infections, osteomyelitis, and myo- and endocarditis can be seen and typically occur in immunocompromised patients as a results of hematogenous spread.1 Treatments includes ampicillin with or without an aminoglycoside. Occasional resistance to tetracyclines has been reported.2
Regarding the patient’s Listeria bacteremia, the patient reported no exposures to the common carriers of Listeria. It is possible that is was translocated from his gut during his diarrhea illness or could have been the cause of his diarrhea, although blood cultures at the outside hospital were negative.
References
- Winn, Washington C., et al. Color Atlas and Textbook of Diagnostic Microbiology. Lippincott Williams & Wilkins, 2006.
- Tille, Patricia M. Bailey & Scotts Diagnostic Microbiology. 13th ed., Elsevier, 2014.
-Casey Rankins, DO, is a 1st year Anatomic and Clinical Pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
