Case History
A 3 year old Caucasian male presented to the hospital due to a gastrointestinal illness and severe dehydration. Per parents, the patient started having diarrhea 4 days prior to admission. Initially, the diarrhea was watery, yellow, and foul-smelling but then became bloody and intermixed with clots. Diarrhea episodes were occurring every 20 minutes and associated with severe abdominal cramping. Additional symptoms included vomiting and malaise, but no fever was noted. There was no history of travel and no one else in the family or at daycare had similar symptoms. On physical examination, there was diffuse abdominal tenderness, signs of dehydration and altered mental status. Vitals showed an elevated blood pressure (144/97) and tachycardia (140 beats/minute). Initial lab work revealed a marked leukocytosis with left shift (78.9 TH/cm2, 62% neutrophils, 11% bands), normal hemoglobin & hematocrit, and a slight thrombocytopenia (156,000 TH/cm2). Notably, the renal panel showed kidney injury (BUN 79 mg/dL and creatinine 3.29 mg/dL) and a significantly elevated LDH (9,408 U/L). Blood and stool specimens were collected for culture and the patient was started on fluids for rehydration therapy.
Laboratory Identification

The isolate was identified as Escherichia coli O157 by Vitek and latex agglutination was positive. Additionally, the patient had a GI PCR panel performed which was also positive for E. coli O157 and Shiga-like toxin-producing E. coli stx1/stx2. The specimen was sent to the department of health which also confirmed the identification of E. coli O157:H7 by molecular methods. All blood cultures remained negative. Based on the clinical presentation and culture results, the child was diagnosed with hemolytic uremic syndrome (HUS).
Discussion
Escherichia coli is a gram negative rod that a member of the Enterobacteriaceae family. General features of the genus include fermentation of glucose, a negative oxidase reaction, and most strains having the ability to ferment lactose. E. coli is a normal component of gastrointestinal flora, but pathogenic strains can cause illness due to ingestion of contaminated food or water, contact with animals, or person to person spread. In the case of E. coli O157:H7, the infectious dose can be as small as 10-100 CFU.
The clinical syndromes caused by E. coli O157:H7 are commonly referred to as Shiga toxin-producing E. coli (STEC) or enterohemorrhagic E. coli (EHEC). Most commonly, E. coli O157:H7 is due to ingestion of undercooked ground beef. Presentations can range from mild non-bloody diarrhea to severe hemorrhagic colitis with hemolytic uremic syndrome (HUS). HUS is characterized by a hemolytic anemia, decreased platelets and organ damage, including renal failure and altered mental status. While only 4% of those infected with E. coli O157:H7 develop HUS, at least 80% of HUS cases in North America are due to E. coli O157:H7.
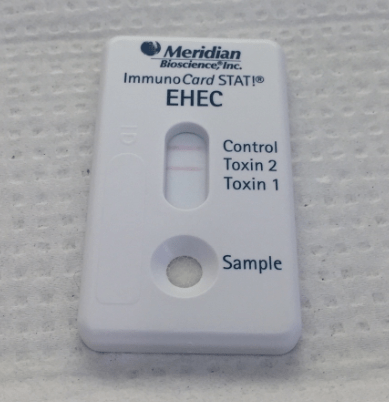
When a stool culture in received in the laboratory, a selective and differential agar to identify E. coli O157:H7 is always used. This is due to the fact that the majority E. coli O157:H7 do not ferment sorbitol. If a sorbitol negative E. coli is identified, latex agglutination is used to confirm the isolate is O157. In addition, lateral flow assays for the detection of the Shiga toxin 1 & 2 proteins are also performed as part of the routine stool culture to detect E. coli isolates that ferment sorbitol or are serotypes other than O157. Molecular testing to detect Shiga toxins provides a sensitive method of detection with an improved turnaround time. Presumptive isolates should be sent to the state department of health for confirmation and monitoring of potential outbreak situations.
Treatment for E. coli O157:H7 is generally supportive as it has been reported that certain antibiotics may stimulate further toxin production, thereby increasing the risk of HUS and as such, no routine susceptibility testing is recommended for STEC strains. Patients may need dialysis in the event of renal failure.
In the case of our patient, he had a prolonged disease course that necessitated dialysis and was complicated by a bowel perforation and pancreatitis. While his condition improved, he still requires dialysis three times a week.
-Aljunaid Alhussain, MD, is a first year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the Director of Clinical Pathology as well as the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement, and resident education.
