Case History and Laboratory Findings
A 24 year old male presented to an urgent care clinic with the complaint of painful pustules on his scrotum for the past 4-5 days. He claims that he had not had any recent exposure to sexually transmitted diseases (STD) or to new sexual partners. A month prior to presentation, he was seen for STD evaluation and was treated empirically for suspected exposure. Testing at that time was negative. The patient was unsure if these pustules were exacerbated by his work, in which he is in tight, hot spaces doing manual labor. His review of systems was otherwise negative. A swab of one of the pustules was sent for gram stain and culture which showed the following:
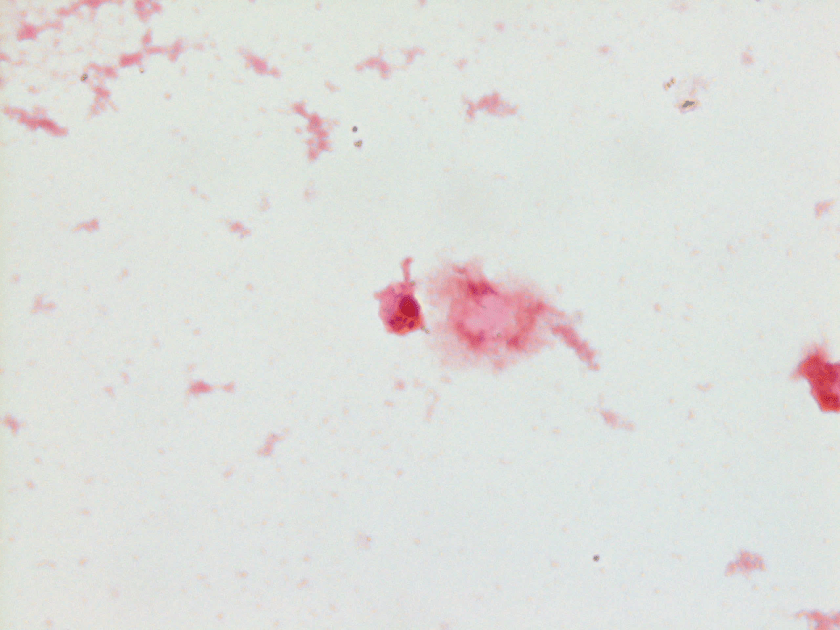

MALDI-TOF identified the organism to be Neisseria gonorrhoeae.
Discussion
N. gonorrhoeae is a gram negative diplococci and the second most common cause of sexually transmitted infections in the United States. The diplococci are described as having adjacent flattened sides giving it the appearance of the letter “D”. N. gonorrhoeae is classically described as a fastidious organism, requiring specialized media (Chocolate, modified Thayer-Martin, Martin-Lewis, New York City agar, etc.) and an enhanced CO2 environment in order to grow, though it is also known to grow on blood agar. Colonies are small to medium in size and are described as flat, grey-brown, and moist. Biochemically, N. gonorrhoeae is catalase and oxidase positive, and is a glucose fermenter.
Neisseria gonorrhoeae can infect the epithelium of the urethra, cervix, pharynx, rectum, and conjunctiva. Infection at these sites results in pain, irritation, and purulent discharge. Dissemination to other locations, such as the skin and joints, can also occur. Though dissemination is uncommon, associated symptoms include: skin sores, fever, migratory polyarthritis, tenosynovitis, and pauciarticular septic arthritis. N. gonorrhoeae infections typically present as acute urethritis with associated discharge. Infections are symptomatic in 10% of males and upwards of 70% of females, putting females at a higher risk of developing ascending infections, and potentially, pelvic inflammatory disease. Disseminated infections occur much less commonly, happening in 0.5% to 3% of all gonococcal infections. Therapy guidelines recommend treating uncomplicated infections with intramuscular ceftriaxone and oral azithromycin. Treatment of disseminated infections is variable depending on patient symptoms, but can include a combination of ceftriaxone/cefotaxime and azithromycin/doxycycline, with variable route of administration and length of treatment times. Susceptibility testing is limited to testing for beta-lactamase activity, though in cases of suspected resistance, CLSI guidelines are available for further testing.
References
- McCormack WM, Stumacher RJ, Johnson K, Donner A. Clinical spectrum of gonococcal infection in women. Lancet 1977; 1:1182.
- Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015; 64:1.
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, 2015. Atlanta, GA: US Department of Health and Human Services; October 2016.
-Clayton LaValley, MD is a 2nd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
