Case History
A 73-year-old man presents to his primary care provider during the height of a bad influenza season with fever, lethargy, and chills. Symptoms started 24 hours prior to presentation. A rapid influenza rapid test was performed in the physician’s office and the result was negative for influenza A and B. What is the most likely cause of this man’s illness?
Answer
Influenza…but how can that be?
Discussion
Rapid antigen testing has been the mainstay for influenza testing since the 1980’s. These tests detect influenza A and B viral nucleoprotein antigens in respiratory specimens, giving a qualitative “positive” or “negative” result. Antigen testing was developed to shorten the turnaround time to results for common respiratory viruses influenza and respiratory syncytial virus (RSV), with an assay run time of approximately 15 minutes compared to the several days it takes for influenza detection by viral culture. Rapid antigen testing is very easy to perform, allowing CLIA-waived testing to be performed at point-of-care.
Unfortunately, rapid antigen testing has poor sensitivity. The most comprehensive analysis found the sensitivity of rapid antigen testing to be around 60% in adults and slightly higher (although still not good) in children. Due to the poor sensitivity, the CDC recommends only employing rapid antigen testing when the prevalence of influenza in the community is >10%…but why does the prevalence matter? Knowing the prevalence of a disease in your population allow you to calculate the positive and negative predictive value.
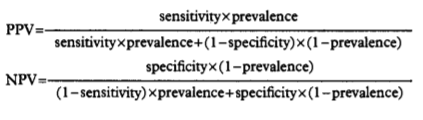
Positive and negative predictive values answer the question, “What is the chance that my positive test result means my patient has the disease (PPV) or what is the chance that my negative test result means my patient does not have the disease (NPV).” You can calculate the PPV or NPV of any assay by knowing the sensitivity and specificity of an assay along with the prevalence of disease in the community (Figure 1).
Positive and negative predictive values fluctuate with the amount of disease seen in a community. For example, if testing for polio in the United States, where the virus has been eradicated, a positive test result by any method is far more likely to be a false-positive than a true-positive result. This is due to the low positive predictive value (PPV) of a positive test result in the setting of non-existent polio. The converse is true for negative predictive values (NPV). In the height of influenza season, a negative test result for influenza in a patient with signs and symptoms of influenza disease is more likely to be a false-negative than a true-negative result.
For influenza rapid antigen testing, the PPV is highest when influenza activity in the community is high (positive test result is likely to indicate influenza infection) and the PPV is lowest when influenza activity is low in the community is low such as in summer, when a positive influenza test result is most likely to be a false-positive result.
Conversely, NPV is highest when influenza activity is low in a community, and a negative test result is most likely indicating that the patient does not have influenza infection. NPV is lowest when influenza activity in a community is high, and a negative test result is more likely to indicate a false-negative result in a patient with influenza infection.
The specificity of rapid antigen assays is tied to the circulating influenza viral subtypes in a given season, and is generally quite high. Sensitivity and specificity do not change due to the prevalence of disease in the community, unlike positive and negative predictive values.
References:
- Centers for Disease Control and Prevention (CDC) website on influenza testing (https://www.cdc.gov/flu/professionals/diagnosis/clinician_guidance_ridt.htm)
- Altman Douglas G, Bland J Martin. Statistics Notes: Diagnostic tests 2: predictive values BMJ 1994; 309 :102
- Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of Rapid Influenza Diagnostic Tests: A Meta-analysis. Ann Intern Med. 2012;156:500–511.doi: 10.7326/0003-4819-156-7-201204030-00403

-Erin McElvania, PhD, D(ABMM), is the Director of Clinical Microbiology NorthShore University Health System in Evanston, Illinois.

Excellent article! And fitting topic given the prevalence of flu this season. Thank you for sharing.