Case History
The lab received a purulent fluid from a frontal subdural empyema in a 56 year old woman with a several month history of sporadic bloody to purulent vaginal discharge and a two week history of severe headache, facial weakness, and recent dysarthria causing her to seek treatment. Pelvic exam and CT of the abdomen revealed a fungating cervical mass, later found to be adenocarcinoma, with possible fluid collection within the uterine cavity.
Lab Identification
Initial gram stain of the subdural fluid showed moderate neutrophils and no bacteria. The aerobic plate showed no growth at 48 hours. The thioglycollate broth grew “puffballs” containing long gram negative bacilli with tapered ends.

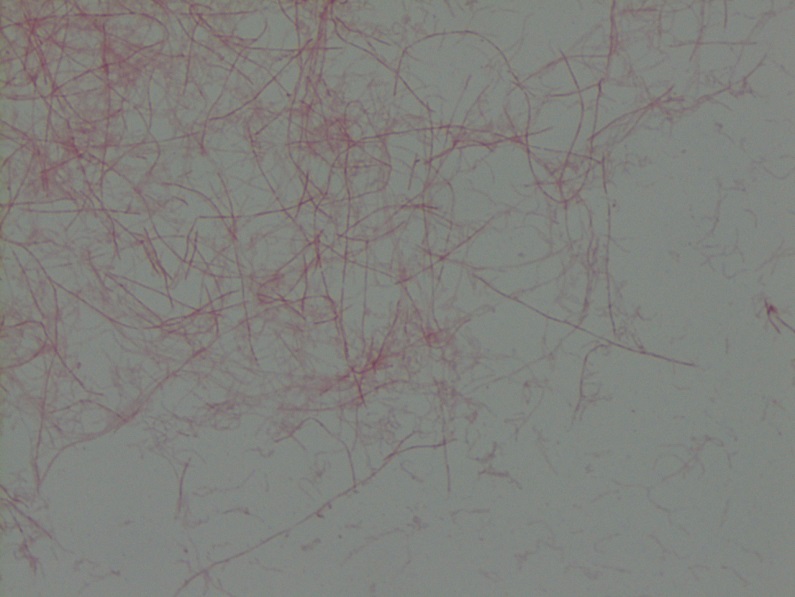
The anaerobic plate grew few grey colonies composed of similarly-shaped gram negative bacilli. MALDI-TOF mass spectrometer identified both colony morphologies as Fusobacterium nucleatum.
Discussion
F. nucleatum is a gram negative, spore non-forming, asacchrolytic, slow-growing, obligate anaerobe that can fluoresce chartreuse under UV light. It is one of 14 species within the Fusobacterium genus and is further classified into 5 subspecies (nucleatum, animalis, fusiforme, vincentii, and polymorphum) which have different pathogenic profiles. It is commonly associated with the oral cavity, though it is unclear if it is ever a constituent of usual flora. Its main virulence factors are invasion of epithelial and endothelial cells, induction of host immune response, and adhesion to tissue through a variety of adhesins. The FadA adhesin interacts with the ubiquitous cell junctional cadherins leading to increased permeability of the epithelial and endothelial barrier. This interaction may be why F. nucleatum infections can be found in such diverse locations within the body and are often part of a polymicrobial infection [1, 2].
F. nucleatum is a constituent of oral plaque and is strongly associated with gingivitis and periodontitis. It is present in increased quantity with increasing severity of disease and in patients with a history of smoking or uncontrolled diabetes mellitus. It is a known pathogen in infections and abscesses of the head and neck, brain, lung, abdomen, blood, and pleura. It is also commonly found in placental and fetal tissues and strongly associated with a variety of obstetrical conditions including preterm birth, chorioamnionitis, and neonatal sepsis. It has been implicated in at least one case as the causative agent of stillbirth. Its prevalence in cord blood in cases of neonatal sepsis is equal to or greater than that of E. coli and Group B Strep. There is also a known association between F. nucleatum and colorectal cancer and IBD, with current research investigating whether the bacteria could play a role in pathogenesis. [1].
F. nucleatum is generally responsive to treatment with a range of antimicrobials, though there are reports of strains resistant to clindamycin and beta-lactamase-based resistance to ampicillin [2, 3].
The infectious disease clinician covering the present case suggested that the patient may have been transiently bacteremic due to her fungating gynecologic malignancy and suffered a minor head trauma causing a small subdural hemorrhage that seeded the bacteria in a sufficiently protected anaerobic environment.
References
- Han TW. Fusobacterium nucleatum: a commensal-turned pathogen. Curr Opin Microbiol. (2015) 23:141-147.
- Denes E, Barraud O. Fusobacterium nucleatum infections: clinical spectrum and bacteriological features of 78 cases. Infection (2016) 44:475-481.
- Veloo ACM, Seme K, Raanges E, Rurenga P, Singadji Z, Wekema-Mulder G, van Winkelhoff AJ. Antibiotic susceptibility profiles of oral pathogens. Intl J Antimicrob Agents. (2012) 40:450-454.
-Taylor Goller is a Pathology Student Fellow at University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Associate Professor at the University of Vermont.
