Case History
The lab received two sets of blood cultures drawn at the time of admission from an elderly woman presenting with escalating signs of shock in the setting of suspected ischemic bowel. An exploratory laparotomy led to resection of a gangrenous segment of large bowel without signs of perforation or abscess. The woman’s medical history in the previous three months included two episodes of GI bleed, including one associated with signs of ischemic bowel, treated conservatively, and a hospitalization for health care acquired pneumonia treated with levofloxacin and steroids.
Lab Identification
Bacterial growth was detected in two bottles from one site. The anaerobic bottle demonstrated gram negative bacilli. The aerobic bottle demonstrated gram positive cocci that were identified by the Verigene microarray as non-VRE Enterococcus faecium. However the Verigene system could not identify the gram negative rod.
The gram negative rod grew on blood, chocolate, and McConkey agar. It was a lactose non-fermentor. Additionally, the gram negative colonies were indole positive and oxidase negative.
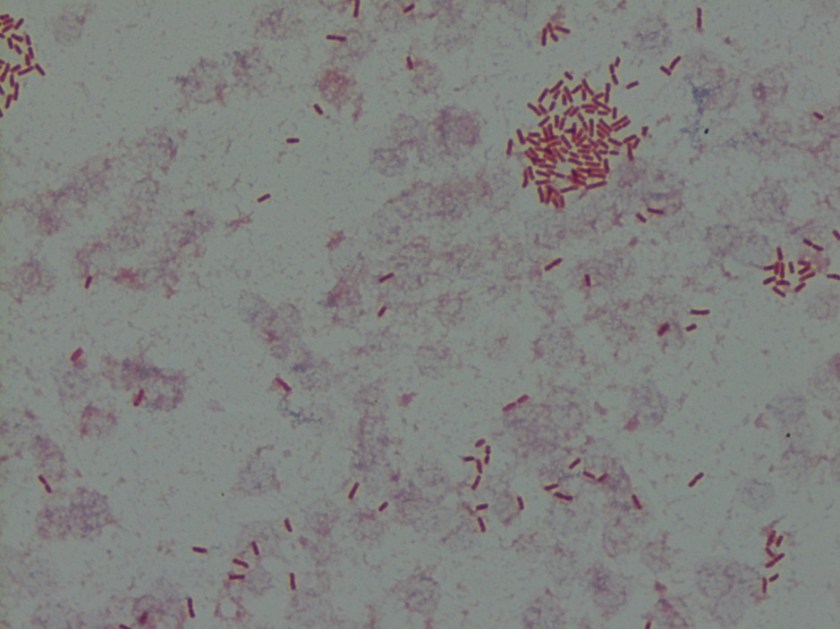
Image 1. Gram stain of anaerobic blood culture bottle.


These colonies were identified by the MALDI-TOF mass spectrometer as Escherichia fergusonii.
Discussion
Originally described as a unique species in 1985, Escherichia fergusonii is the closest relative of the much more common and well-known Escherichia coli.1 It is differentiated from E. coli by being lactose and sorbitol negative but adonitol, amygdalin, and cellobiose fermentation positive. Due to its molecular and structural similarities to E. coli, platforms such as the MALDI-TOF or Vitek 2 may have difficulty discriminating between the two species.2, 3 It has been identified as normal intestinal flora of warm blooded animals, though not specifically humans, and has been implicated in a salmonellosis-like disease in sheep and cattle.3
Descriptions in the literature regarding the clinical relevance of E. fergusonii to human disease are limited. There have been reports of E. fegusonii acquiring known virulence factors from E. coli and Salmonella, however, the prevalence and significance of such transformation is not well understood. In one report, E. fergusonii was found to have acquired the E. coli O157 antigen, but did not acquire the associated virulence factors or Shiga toxin.4 It has been identified as the pathogenic agent in cases of urinary tract infection, wound infection, diarrhea, bacteremia, cholangiosepsis, pleuritis, and endopthalmitis. These reports are geographically widespread with E. fergusonii identified in patients from the US, Nicaragua, Italy, India, and Taiwan. There is also variable information on antimicrobial susceptibility. The original description by Farmer et al. reported that all strains were susceptible to colistin, gentamicin, and chloramphenicol, and resistant to penicillin.1 An analysis of 600 specimens from eastern India revealed high rates of resistance to gentamicin and chloramphenicol and moderate resistance to ampicillin.5 An analysis of urinary tract infection specimens from Nicaragua reported resistance to nitrofuratoin, ciprofloxacin, ceftriaxone, and amoxicillin-calvulanate.6
Interestingly, E. fergusonii has been identified as the most quickly evolved member of the Escherichia genus.7 Though it is unclear whether that rapidity of differentiation translates to an ability to acquire clinical relevant features, it can at least be concluded E. fergusonii is a widely distributed and possibly under-identified gram negative facultative bacillus with the potential to acquire virulence factors and antibiotic resistance that could make it a significant pathogenic organism in humans.
References
- Farmer JJ, Fanning GR, Davis BR, O’Hara C, Riddle C, Hickman-Brenner FW, Asbury MA, Lowery VA, Brenner DJ. Escherichia fergusonii and Enterobacter taylorae, two new species of Enterobacteriaceae from clinical specimens. J. Clin. Microbiol., 21 (1985): 77–81.
- Crawford-Miksza LK, Himathongkam S, Dodd ML, Badoiu AS, Badoiu OM, Guthertz LS. Misidentification of a variant biotype of Escherichia coli O157:H7 as Escherichia fergusonii by Vitek 2 compact. J. Clin. Microbiol., 47 (2009): 872–873.
- Gastra W, Kusters JG, van Duijkern E, Lipman LJA. Escherichia fergusonii. Vet. Microbiol., 172 (2014): 7-12.
- Fegan N, Barlow RS, Gobius KS. Escherichia coli O157 somatic antigen is present in an isolate of E. fergusonii. Curr. Microbiol., 52 (2006): 482–486.
- Mahapatra A, Mahapatra S, Mahapatra A. Escherichia fergusonii: an emerging pathogen in South Orissa. Indian J. Med. Microbiol., 23 (2005): 204–208.
- Bours PHA, Polak R, Hoepelman AIM, Delgado E, Jarquin A, Matute AJ. Increasing resistance in community-acquired urinary tract infections in Latin America, five years after the implementation of national therapeutic guidelines. Int. J. Infect. Dis., 14 (2010): e770–e774.
- Walk ST, Alm EW, Gordon DM, Ram JL, Toranzos GA, Tiedje JM, Whittam TS. Cryptic lineages of the genus Escherichia. Appl. Environ. Microbiol., 75 (2009): 6534–6544.
-Taylor Goller is a Pathology Student Fellow at University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.

I’m so glad I found this blog! In just a few short weeks I have learned so much about pathogenic microorganisms!