Case History
A 50 year old male initially presented with cold symptoms. He was seen and evaluated at urgent care, with suspicion for bronchitis, but with no improvement with albuterol. Physical exam raised a suspicion for bacterial sinusitis. The patient was treated with amoxicillin/clavulanic acid with little improvement, and he was admitted to the hospital a week later for fever and diarrhea. Blood cultures were obtained. He was initially treated with cefepime prior to the speciation of the culture, and then switched to erythromycin for a 7 day course.
Laboratory Identification
Blood cultures were positive for gram negative curved/spiral rods. Gram stain and colony morphology were consistent with Campylobacter which was confirmed as C. jejuni by MALDI-TOF.
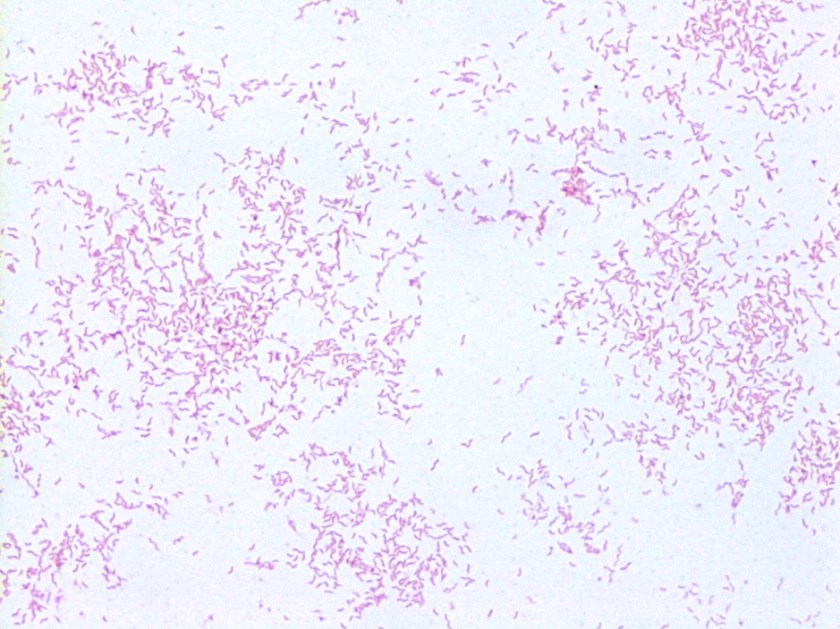
Image 1. Gram stain showing gram negative curved/spiral rods.
Discussion
C. jejuni are gram negative curved or spiral rods. Campy CVA agar is used for stool cultures because it is selective for Campylobacter and contains cefoperazone, vancomycin, and amphotericin B (CVA) which inhibit normal fecal flora. The media is incubated at 42°C under microaerophilic conditions, supporting the growth of Campylobacter jejuni and C. coli. C. jejuni is thermophilic, with growth on blood agar at 37°C and 42°C. Growth does not occur at 25°C. The colonies on blood agar are non-hemolytic, gray and smooth. Our isolate grew, albeit not happily, on blood and chocolate at 37°C with 5-10% CO2.
Infection is often transmitted by contaminated foods such as undercooked chicken. C. jejuni are most commonly associated with human infections however, C. coli have also been implicated. Guillain-Barre syndrome has been associated with patients following an infection with C. jejuni. It is not known how our patient was exposed. Macrolides are effective treatment modalities for C. jejuni, as well as fluoroquinolones, however, resistance to fluoroquinolones is increasing.
-Mustafa Mohammad, MD is a 3rd year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.

As part of a microbiology course I am taking, our instructor wants us to interact with the author of a microbiology blog. I do have a question concerning this case: Was this a case of an opportunistic infection occurring due to an already compromised immune system, or is it possible this infection was present the entire time? Thanks!
Hi Vanessa, Sounds like you are in a pretty fun micro course! To my knowledge, this patient was not immunocompromised. According to Mandell’s Principals and Practice of Infectious Diseases bacteremia is present in about 1% of patients with C. jejuni infection. This might be a low estimate as most patients with diarrhea do no get blood cultures drawn. It usually is seen in people at the extremes of age. There are thought to be 3 patterns of bacteremia with C. jejuni: transient bacteremia in a normal host (usually getting better by the time blood culture results are completed), sustained bacteremia or deep focus of infection in a normal host (usually patients have acute enteritis), and sustained bacteremia or deep focus of infection in a compromised host (many patients do not have acute enteritis). My thinking on our patient was his initial presentation with sinusitis symptoms was unrelated to his C. jejuni infection. He likely had a transient bacteremia. I hope this helps!
This helps me immensely! Thanks so much for taking the time to write such an informative reply! We’ve not seen “Mandell’s Principals and Practice of Infectious Disease” yet, unless the standards are commonly known by another name or are just taught, but I think you’ve just given me the topic for my term paper! Thanks so much!
Antibiotic associated diarrhea, Can we label this case as antibiotic associated diarrhea ? Because previous antibiotic destroy the normal intestinal flora (of course long term antibiotic -more than 2 weeks) and then the injured intestinal flora is a ‘fertile land’ for Campylobacter, Clostridium defficile like organisms.