Case History
A 25 year old Caucasian male with no significant past medical history presented to the emergency department (ED) with a several day history of persistent fevers, headache (pain 10/10), dizziness and neck pain. He also reported facial and hand numbness and difficulty focusing at work. His laboratory values at that time showed a normal white blood cell count (5.3 TH/cm2), normal hemoglobin (13.8 g/dL), slightly decreased platelet count (142,000 TH/cm2) and slightly elevated liver enzymes. A computed tomography (CT) of his head showed no abnormalities, and a lumbar puncture was performed that was suggestive of viral meningitis (92% lymphocytes). After obtaining blood cultures, the patient received a dose of vancomycin and ceftriaxone and was discharged home.
Two days later he returned to the ED with complaints of worsening neck pain, photophobia, decreased appetite, and fevers reaching 105°F. He reported fevers of such intensity that he resorted to soaking himself in ice baths. On further questioning, he reported working in a microbiology lab that handles cytomegalovirus (CMV) and attenuated mycobacterium, but was unaware of any exposures or sick contacts. He has 2 dogs he rescued (one with a history of heartworm), 3 cats (one with a history of tapeworms) and a mouse. Infectious disease was consulted and a thorough workup was initiated, which included repeat blood cultures and testing for hepatitis, human immunodeficiency virus (HIV), respiratory pathogens and syphilis. He was started on cefepime initially and then later changed to meropenem and levofloxacin.
Laboratory identification
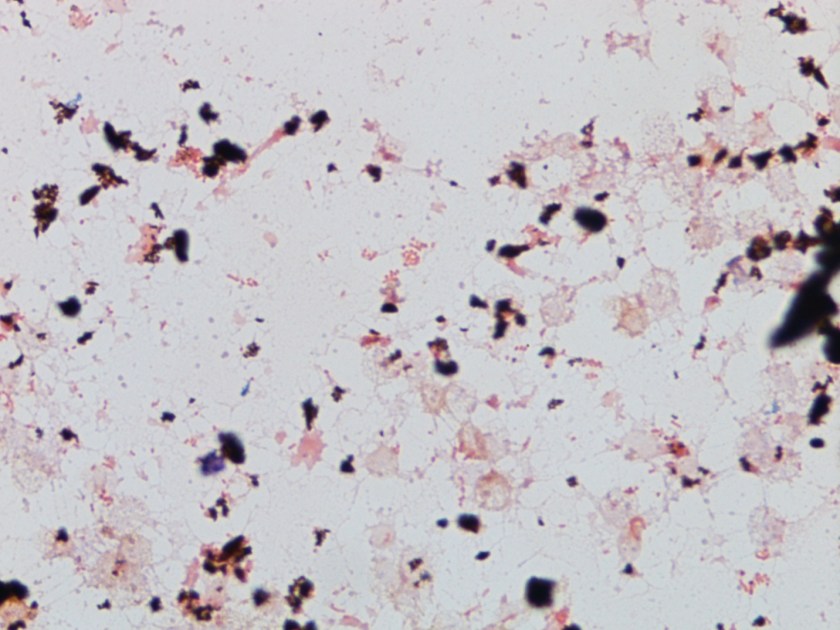
Figure 1. Gram stain from a positive blood culture illustrating small Gram negative coccobacilli (100x, oil immersion).
The microbiology laboratory reported the blood cultures collected during his second hospital visit were positive with small gram negative coccobacilli after approximately 60 hours on the automated instrument (Figure 1). No growth was noted after 24 hours incubation at 35°C in 5% CO2 on standard media. After 48 hours, small white colonies grew on sheep blood and chocolate agars but failed to grow on MacConkey agar. Biochemical tests revealed the organism was positive for catalase, oxidase and urease. In accordance with the suspected agents of bioterrorism manual, the culture was sent to the State Department of Health for further classification. The organism was identified by PCR as Brucella spp. Subsequently, the Centers for Disease Control and Prevention (CDC) performed species level PCR and identified the isolate as B. canis.
On further questioning, the patient denied consuming unpasteurized milk products but reported recently adopting a pregnant dog from a local shelter, who had subsequently delivered stillborn puppies of which the patient had been in close proximity. At this point, the patient’s antibiotics were switched to a 6 week course of oral doxycycline and rifampin. On follow up visits, he was doing well and symptom free. Unfortunately, the dog also tested positive for B. canis and had to be euthanized.
Discussion
Brucella spp. are common zoonoses among wildlife and domestic animals including cattle (B. abortus), pigs (B. suis), goats (B. melitensis) and dogs (B. canis) who are usually asymptomatic carriers. While rare in the United States due to vaccination of livestock, Brucella spp. is considered endemic in areas of the Middle East, Central and South America and the Indian subcontinent. Symptoms of infection generally occur during an infectious abortion in which the placenta, fetal tissues and secretions contain high levels of the bacteria which can survive in the environment under various conditions for long periods of time. Humans are usually infected due to consumption of unpasteurized milk and cheeses. High risk professions such as veterinarians and slaughterhouse workers can also be infected by direct contract with contaminated materials or inhalation of aerosolized particles. Symptoms generally appear 1 to 2 weeks after infection with remittent/undulant fever the characteristic feature of the illness, in addition to arthralgias, fatigue, weight loss and hepatomegaly.
Laboratory identification of Brucella spp. is the gold standard but can be challenging as it is a slow growing organism and can infect personnel leading to laboratory acquired infections (LAI). When small Gram negative coccobacilli are identified that fail to grow on MacConkey agar, this should alert the laboratory worker of a potential agent of bioterrorism and work up should be performed in appropriate biosafety cabinets. Brucella spp. grows as small, smooth white colonies that appear after 24 to 48 hours incubation. It is catalase, oxidase and urease positive. Automated systems and MALDI-TOF mass spectrometry are not terribly reliable or recommended for identification of this organism due potential aerosolization events. When Brucella spp. is suspected, the level A clinical laboratory (a sentinel lab) should notify and send samples to a Level B/C lab (state health department) for confirmation. Subsequently, confirmed isolates can be forwarded to a level D lab (CDC) for speciation.
While overall, the mortality for Brucella spp. is very low, significant morbidity can result with long term non-specific symptoms and cardiac and osteoarticular complications. Good outcomes result when acute presentations are treated with combined regimens of antibiotics. The World Health Organization (WHO) recommends the use of oral doxycycline and rifampin for 6 to 8 weeks. Susceptibility testing is not recommended as resistance is rare and the concern for laboratory safety. In the case of laboratory exposures, prophylaxis with doxycycline and rifampin for 3 weeks is recommended for high risk workers. In the case of low risk employees, temperature monitoring for 6 months and serologic testing at defined time points is standard as the incubation period for Brucella can be this long.

-Melissa Brents, MD, is a 4rd year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.

Excellent. Case history was very well written and reported.