Case History
A 57 year old female presents to the hospital with complaints of a recurrent fever for the past few days. Her past medical history is significant for acute myeloid leukemia (AML). On physical examination, she has multiple, warm, erythematous, non-painful papules and nodules involving her extremities. One of the lesions, located on the dorsal aspect of her finger, had ulcerated. She is found to be neutropenic with a white blood cell count of 0.36 TH/cm2 (reference range 4.0-10 TH/cm2). A chest CT scan is performed and reveals multiple, small hyperdense pulmonary nodules. As part of the work up for febrile neutropenia, blood cultures are collected. Dermatology was also consulted and a skin biopsy at the advancing edge of the lesion was performed.
Laboratory Identification

Figure 1. Review of the deep portion of the punch biopsy demonstrates panniculus with a deep, dilated vessel containing fibrin and possible fungal organisms (H&E, 40x).

Figure 2. Deep dilated blood vessel with fibrin and fungal forms consistent with a hyaline septate mold were identified (H&E, 400x). Mycotic organisms were confirmed by a Grocott’s methenamine silver (GMS) stain.

Figure 3. Gram stain from a positive blood culture vial highlighting narrow hyphal elements with acute angle branching consistent with a hyaline septate mold (400x).
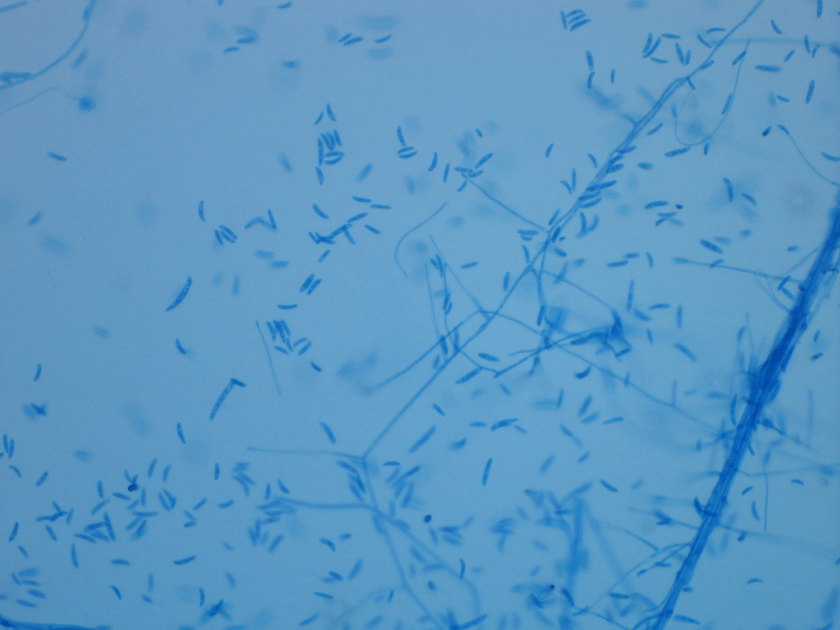
Figure 4. Lactophenol cotton blue preparation highlighting septate hyphae and numerous macroconidia that can be described as canoe or banana shaped (400x).
All of the specimens were collected on the same day and the results from the skin biopsy which showed fungal elements consistent with a hyaline septate mold were reported first (Figure 1). After 2 days of incubation, multiple blood culture bottles were positive for a mold similar to what was seen on tissue biopsy, indicating a disseminated fungal infection in this severely immunocompromised patient (Figure 2). Fungal cultures were set up from the blood and after 5 days of incubation at 30°C, lavender cottony colonies with lighter periphery grew on Sabouraud’s dextrose agar (SDA). The lactophenol cotton blue preparation showed many macroconidia with three to five septa (Figure 4). All of the findings are consistent with Fusarium spp.
Discussion
Fusarium spp. are filamentous fungi which are classified as a rapidly growing, hyaline septate mold. This opportunistic mold can be found all over the United States in the soil and on plants. In immunocompetent individuals, Fusarium spp. can cause localized infections, most commonly as the result of traumatic inoculation. Frequently, the eye is the site of infection, leading to keratitis. This can be due to trauma, contamination of contact lenses or solution, or corticosteroid drops. Fusarium has been reported as the infectious pathogen and has many clinical manifestations such as pneumonia, sinusitis, and wound infections. However, in immunocompromised patients, Fusarium spp. pose a greater threat for invasive and disseminated infections. Of the fungal organisms routinely implicated in fungemia (in addition to Candida, Cryptococcus and Histoplasma), Fusarium spp. have a high frequency of positive blood cultures.
Blood cultures positive for a septate mold and the presence of characteristic skin lesions are highly indicative of a disseminated Fusarium infection, especially in a severely neutropenic patient. To support the diagnosis of fusariosis, it is reassuring to have two different specimens each growing the same pathogen. In the case of our patient, both blood and skin tissue cultures grew Fusarium spp. with the same colony and microscopic morphology. The patient was unable to produce sufficient sputum for respiratory cultures, but the lung abnormalities were attributed to the fungal process as well.
In the laboratory, Fusarium spp. grow relatively rapidly on Sabouraud’s dextrose agar and can usually be identified within 3 to 5 days. Colonies are typically cottony in appearance and develop a pink to lavender color as they mature. The reverse of the plate is usually light. Fusarium spp. produce both macroconidia and microconidia. The characteristic macroconidia have been described as canoe, banana or sickle shaped and are separated by 3 to 5 transverse septa. The microconidia arise from short conidiophores and are more oval in shape, containing zero to one septa and can be single or arranged in clusters.
In cases of invasive fusariosis, anti-fungal agents such as voriconazole or high-dose amphotericin B are therapies of choice. In the case of neutropenic patients, growth factors (G-CSF or GM-CSF) or granulocyte transfusions are potential treatment options as well. Surgical debridement of necrotic tissue has shown benefit in patients with large abscesses. Additionally, if the cause of the fungemia is thought to the result of an infected line, the catheter should be removed.
Disseminated involvement of Fusarium spp. has a high rate of mortality associated with the infection. Often times the prognosis is related to the extent of infection and the degree immunosuppression. It is important to suspect Fusarium infections in the clinical setting of a severely neutropenic patient with skin lesions and having a low threshold for beginning anti-fungal therapy. An accurate and prompt diagnosis will lead to appropriate treatment and improved outcomes.

-Katie Tumminello, MD, is a fourth year Anatomic and Clinical Pathology resident at the University of Mississippi Medical Center.

-Lisa Stempak, MD, is an Assistant Professor of Pathology at the University of Mississippi Medical Center in Jackson, MS. She is certified by the American Board of Pathology in Anatomic and Clinical Pathology as well as Medical Microbiology. She is the director of the Microbiology and Serology Laboratories. Her interests include infectious disease histology, process and quality improvement and resident education.

couldn’t have explained it better myself!