Case presentation
A 12-year-old female is seen in gastroenterology clinic following 2 weeks of abdominal pain. She is an otherwise healthy child with no significant past medical history. Her abdominal pain was diffuse, but it has worsened in the past 5 days and is now localized to the left upper quadrant and is sharp in nature. The pain was severe enough to prevent her from attending school last week. She was evaluated for appendicitis, which was ruled out. The patient was admitted for further management including an upper and lower endoscopy. During the endoscopy procedure, small, mobile worms were visualized in the ascending colon. Two worms were collected and removed for identification (Figure 1).
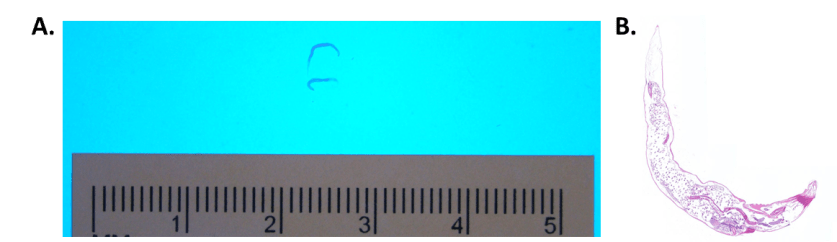
Figure 1. (A) Small, threadlike worms measuring 5-10 mm. Note pointed posterior tail. (B) Haematoxylin and eosin (H&E) stained cross section of the worm.
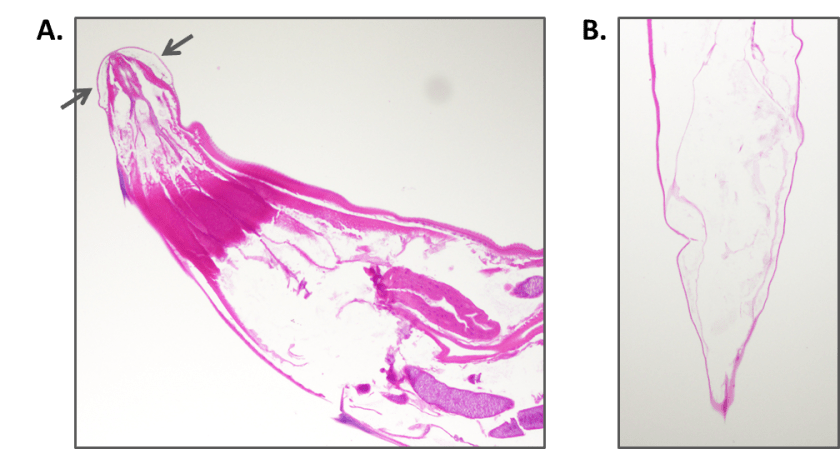
Figure 2. Cross section of the worms shows (A) anterior with cephalic inflations of the cuticle (arrows) and (B) a long pointed tail.

Figure 3. Internal eggs are 50-60 µm x 20-30 µm in size. They are elongated, flattened on one side, and have a thick colorless shell.
Discussion
The worms were identified as Enterobius vermicularis or pinworm. E. vermicularis is a nematode or round worm. Adult worms are 2.5 mm x 0.1 mm (males) and 8-13mm x 0.3-0.5mm (females). Both male and female worms have cephalic inflations of the cuticle at their anterior end (Figure 2A, arrows). Males have a wide blunt posterior tail while females have a long, pointed tail (Figure 1, 2B). Our worms were females as internal eggs were found in both worms. The eggs of E. vermicularis are 50-60 µm x 20-30 µm in size. They are elongated, flattened on one side, and have a thick colorless shell (Figure 3).
E. vermicularis infection is very common in preschool and school aged children as well as families and caregivers of infected children. Transmission occurs through the fecal-oral route. Embryonated eggs are ingested and travel to the small intestine. Adult worms reside in the colon. Gravid females migrate to the anus and deposit eggs onto the perianal area during the night. A single female can deposit as many as 10,000 fertilized eggs. Larvae within the eggs develop and become infective as quickly as 4-6 hours after they are deposited. The entire life cycle from ingestion until eggs are laid by a gravid female in the perianal area is 1-2 months. Perianal scratching and autoinfection are common as well as infection from contaminated fomites such as bedding, clothes, and shared toys.
The most common method of E. vermicularis detection is the Tape Prep method. Briefly, transparent (unfrosted) tape is used to touch the perianal region, after which the tape is placed on a glass slide for microscopic examination. The best time to detect E. vermicularis is 2-3 hours after the patient has gone to sleep due to the nocturnal cycle of the gravid females. Because E. vermicularis does not enter the stool stream, ova and parasite examination often fails to detect the parasite and is not recommended.
Discovery of E. vermicularis in our patient was an unexpected finding, as our patient had no perianal itching. Asymptomatic detection of E. vermicularis has been described in the past, so this finding is not unique. The patient was given a dose of albendazole and will receive another in two weeks, as the drug has reduced effectiveness at killing the eggs or larval stages of development. Her abdominal pain was attributed to overuse of nonsteroidal anti-inflammatory drugs (NSAIDS) and she is being monitored by gastroenterology outpatient clinic.
References
- Ash and Orihel’s Atlas of Human Parasitology, 5th
- Red Book 2015 Report of the Committee on Infectious Diseases, 30th
I would like to thank the staff of the Children’s Medical Center Histology Laboratory for sharing my enthusiasm for parasites as well as sectioning, staining, and taking images of the worms for educational purposes.

-Erin McElvania TeKippe, PhD, D(ABMM), is the Director of Clinical Microbiology at Children’s Medical Center in Dallas Texas and an Assistant Professor of Pathology and Pediatrics at University of Texas Southwestern Medical Center.

Hi Erin…good case…Do you think that E.vermicularis can cause abdominal pain for so long…. children usually not present with such history…is your patient all well……
Thanks
The patient is fairly well and being monitored as an outpatient. It’s most likely that E. vermicularis was an incidental finding and is not the cause of her abdominal pain, because as you mentioned, the symptoms are not consistent with her presentation. The patient had a complicated history including psychiatric issues that I did not mention in the case. This puts her at increased risk for atypical infections as well as many non-infectious causes of abdominal pain.