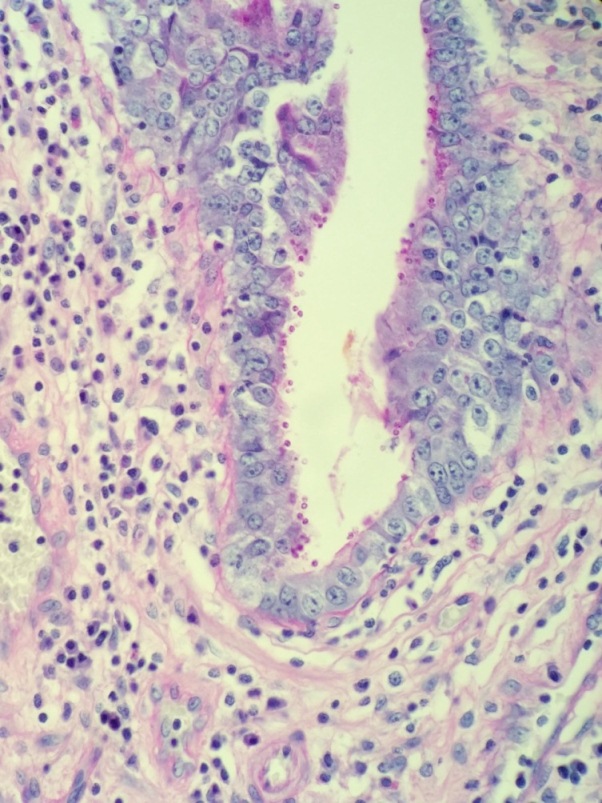
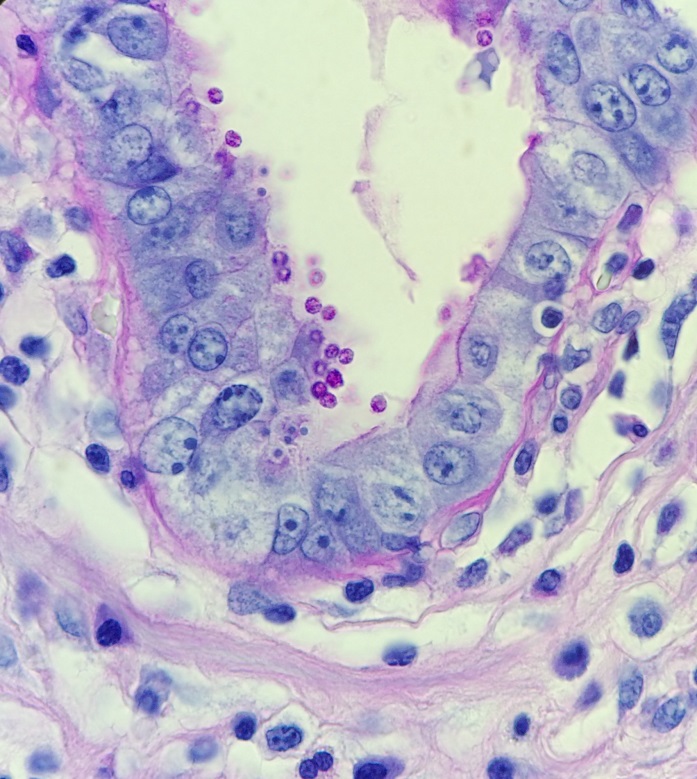
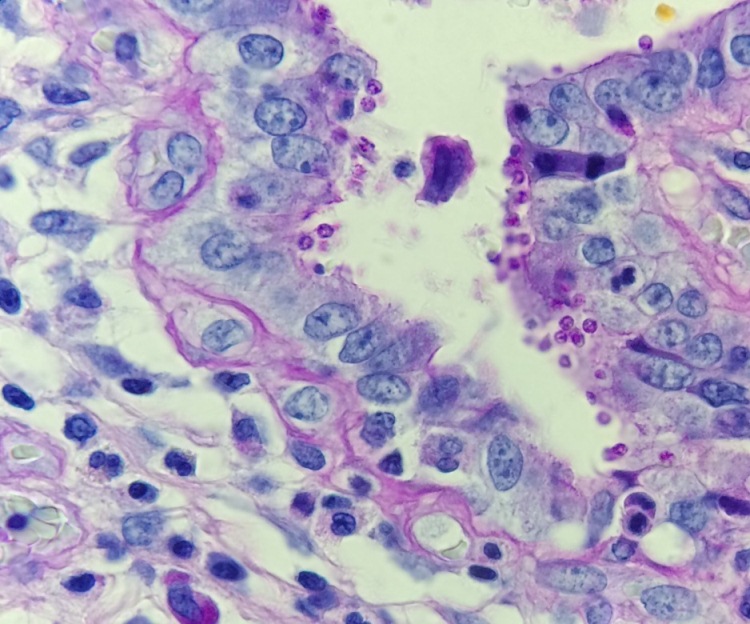
A 43-year-old man with AIDS with a complicated medical history, including multiple recent hospitalizations for CMV esophagitis, recurrent Clostridium difficile, multiple Klebsiella urinary tract infections and pyelonephritis, presented with right upper quadrant pain and profuse watery diarrhea. The ensuing work-up results in a diagnosis of cholecystitis and the patient underwent cholecystectomy. Subsequently, he developed an infected biloma necessitating the placement of a biliary drain. Photomicrographs of his cholecystectomy specimen are shown below.
Laboratory Identification
The diagnosis of cryptosporidiosis was made by H&E section. In a background of acute and chronic inflammation, numerous spherical organisms were identified lining the epithelial surface. Special stains, including PAS and mucin, were performed. The PAS was positive and the mucin stain negative in the organisms. The organisms measured between 2-5 microns. Important differential diagnoses include Cyclospora cayatanesis, which is a bit larger in size (8 microns), Isospora belli, which is much larger (20 microns) and Microsporidia, which is smaller (1-4 microns). Of note, microsporidia appears to be within the apical cytoplasm of mucosal epithelial cells on histology.
While a stool sample was not submitted to the microbiology laboratory in this case, there are several characteristic features of cryptosporidia that should be noted. Importantly, the detection of the oocysts by traditional O&P methods can be very difficult because they can look like yeast which is normal bowel flora. If a clinician suspects cryptosporidiosis, a modified acid fast stain should be performed as cryptosporidia oocyts are weakly acid fast. They also have the ability to autofluorescence when exposed to UV light. More sensitive techniques being used in laboratories today include direct fluorescent antibody [DFA], and/or enzyme immunoassays (ELISAs) for detection of Cryptosporidium sp. antigens.
Discussion
Cryptospoidiosis usually causes watery diarrhea, abdominal pain, nausea, vomiting, fever and weight loss. In a patient with an intact immune system, symptoms usually last 1-2 weeks, and eventually resolve without medical therapy. In an immunocomprimised host such as our patient, however, ingestion can result in severe and even life-threatening disease. Furthermore, use of usual antimicrobial drugs is generally ineffective in this patient population, making them particularly vulnerable.
Cryptosporidium belongs to the taxonomic group Protozoa, phylum Apicomplexa. This group of organisms includes many other important parasites such as Toxoplasma, Plasmodium, Babesia, Cyclospora, and Isopora. The Apicomplexan group is significant for the fact that they possess an apical structure enabling their penetration of host cells. Interestingly, Cryptosporidium is considered to be a eukaryotic intracellular, but extracytoplasmic pathogen as it resides in the columnar brush border of epithelial cells. This particular niche is thought to allow the parasite to evade the immune surveillance while being able to simultaneously take advantage of the solutes transported across the host microvillus membrane. Of the many Cryptosporidium species that exist, Cryptosporidium parvum and Cryptosporidium hominis are the most important in human disease (cryptosporidiosis).
Excretion of thick-walled sporulated oocysts by an infected host results in transmission of the disease through contaminated water sources, such as drinking supplies and recreational water sources. Occasionally contaminated food sources and zoonotic transmission may occur. Importantly, the oocysts are infective upon excretion, thus permitting direct and immediate fecal-oral transmission. Following ingestion, the oocyst excyts in the stomach and then undergo two stages of reproduction within the gastrointestinal tract, an asexual followed by a sexual phase referred to as merogony. Merogony is important in the pathogenicity of many Apicomplexa organisms as it results in massive DNA replication and the creation of hundreds of daughter cells simultaneously.
Cryptosporidia is an important public health hazard because of its resistance to chlorine. Chlorine is often used in water treatment facilities and public water sources as a disinfectant as it kills important pathogens such as Salmonella, Campylobacter, and norovirus. It is ineffective, however, against the thick walled cysts of cryptosporidia. UV light or a filtration system is needed to eradicate cryptosporidium from a contaminated water source.
References
- CDC website, accessed 2/8/2016 http://www.cdc.gov/parasites/crypto/diagnosis.html
- Forbes, B, Sahm, D, Wessfeld, A, Bailey & Scott’s Diagnostic Microbiology, 12th ed. 2007.
- Chalmers, RM, Cryptosporidium: From Laboratory Diagnosis to Surveillance and Outbreaks. Parasite, 2008, 15, 372–378.
-Jessica Crothers, MD is a 4th year anatomic and clinical pathology resident at the University of Vermont Medical Center.

-Christi Wojewoda, MD, is the Director of Clinical Microbiology at the University of Vermont Medical Center and an Assistant Professor at the University of Vermont.

Brillant!!