In a previous post, I mentioned how uncontrolled cell division can occur in any cell type that has the capacity to proliferate, resulting in a neoplasm. Malignancies don’t discriminate – whether the malignant cell is identified within the skin, bladder, breast, bone, muscle, or brain – cancer is cancer. Fortunately, there are many specialists within various disciplines that can identify precancerous changes and other diagnostic abnormalities. Many patients in our head & neck clinic were referred by their dentist who identified a white patch on their tongue, a lump, or a sore that bleeds easily. Similarly, ophthalmologists can recognize ocular lesions during a routine eye exam, and I’m here to share some of those interesting ocular FNA cases. The idea of sticking a needle in your eye is perhaps one of the least pleasant thoughts a person can have, however, these FNAs are crucial for cytopathologists to analyze the cells to confirm a diagnosis.
Depending on the area of the eye sampled and the nature of the lesion, eye FNAs can yield very limited material. Optimal preservation and cytopreparation of ocular samples is imperative. At times, the sample may yield less than 50 cells, from which a diagnosis is expected to be made. Patient history and clinical impression are also crucial to properly triage the FNA. For suspected lymphomas, a portion of the sample should be sent to flow cytometry. For presumed melanomas and metastatic disease, extra preparations should be prepped for immunohistochemistry analysis. In contrast, a clinical impression of a stromal cyst is important to know as these FNAs are likely to be virtually acellular albeit rare cyst contents. The following four cases are presented with their histories and clinical impressions, supplemented by ancillary material.
Case 1. 58 year old male with a history of papillary thyroid carcinoma (2016) and renal cell carcinoma (2018). He presented with periorbital pain and a choroidal mass, OS.
Final Diagnosis: Positive for malignant cells, consistent with metastatic renal cell carcinoma.
Case 2. 58 year old female with a history of breast cancer. She presented with retinal detachment and nonpigmented nodules, OS.

Final Diagnosis: Positive for malignant cells, consistent with metastatic mammary carcinoma.
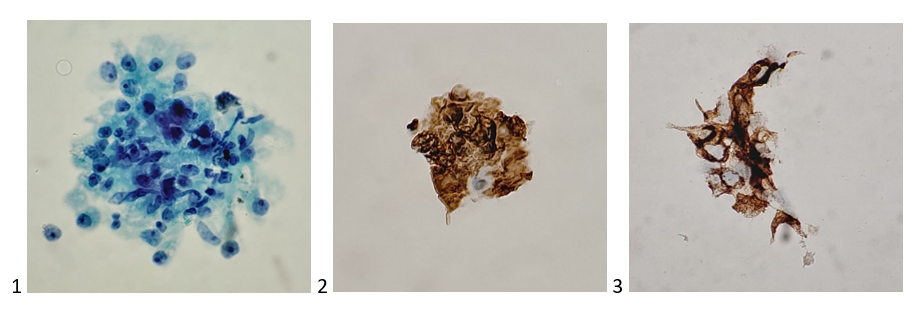
Case 3. 80 year old male with a history of lung adenocarcinoma (2012), pituitary adenoma (2013), and liver carcinoid (2019). He presented with a choroidal lesion, OS.


Final Diagnosis: Positive for malignant cells, metastatic neuroendocrine neoplasm (favor carcinoid tumor).
Case 4. 13 year old male with no cancer history. He presented with a choroidal lesion and retinal detachment, OD. Clinically suspicious for choroidal melanoma.

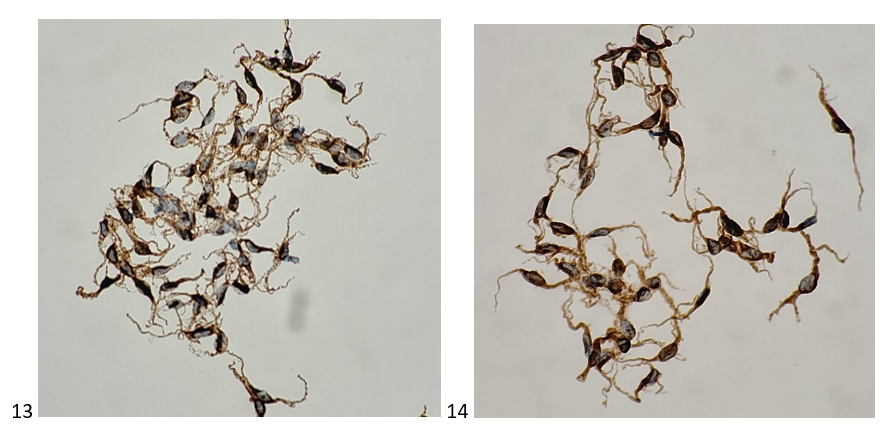
Final Diagnosis: Positive for malignant cells, malignant melanoma (spindle B cell type).
Treatment of eye tumors can range from topical chemotherapies or excision for lesions on the surface of the eye, whereas intraocular tumors can be treated by brachytherapy or evisceration (removing intraocular contents and leaving the scleral shell) or enucleation (complete removal of both the intraocular contents and the scleral shell). While prosthetics are available for the latter therapies, an accurate cytopathology diagnosis is vital to guide treatment in the field of ocular oncology.
Well, that’s all that EYE have for you today. Stay tuned for next month’s cytology case study!

-Taryn Waraksa, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
