A 40 year old man was found deceased in a parking garage in a Midwest city. It was late October and had rained the previous evening. He was identified by his sister who was a tenant in the adjacent apartment building. Unknown to her, he had recently been discharged from the hospital after a one-week psychiatric admission. His sister stated he was homeless and would occasionally sleep in the parking garage for shelter.
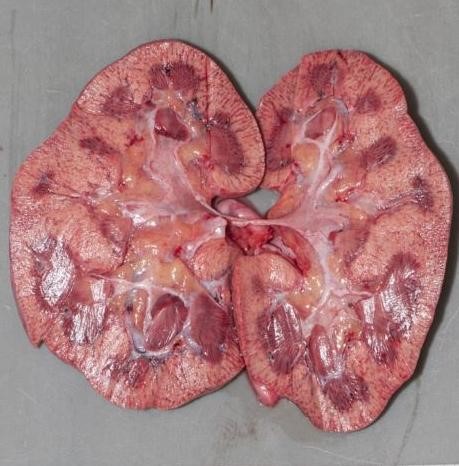
At the scene the decedent was prone on the ground, clad only in a pair of boxers. His water-soaked shoes, socks, sweatpants, and shirt were strewn about him. Autopsy revealed an atraumatic, thin adult man. Prominent pink discoloration was noted over the hips and knees. Internal examination showed only patchy black-brown discoloration of the gastric mucosa and pale kidneys. Histology was remarkable for subnuclear vacuolization of the renal tubular epithelium. The cause of death was certified as environmental hypothermia, and the manner of death accidental.
Hypothermia is defined as a core body temperature below 95℉ (35℃) and can result from endogenous illnesses like hypothyroidism or sepsis. The most common cause, though, is exposure to cold environments. On exposure, the hypothalamus initiates shivering and increases cellular metabolism to produce heat. Another crucial survival response is vasoconstriction, particularly of vessels in skin and skeletal muscle. If the overall loss of heat overtakes the body’s ability to produce or retain heat, hypothermia will result.
Developing hypothermia doesn’t require frigid weather – in dry air, temperatures of 50℉ can still result in hypothermia. Wind removes warmed air surrounding the body, and water conducts heat three times faster than air; therefore, with either of these factors present, people can develop hypothermia at even warmer temperatures,
The autopsy findings of hypothermia are not specific. External examination may show bright pink discoloration of the skin over joints (“frost erythema”). There may be black-brown spots on the gastric mucosa, (“Wischnewsky spots”), thought to result from terminal vasodilation of submucosal vessels. The kidneys may be pale with microscopic subnuclear vacuolization of the tubular epithelium (the “Armanni-Ebstein” lesion). Acute hemorrhagic pancreatitis has also been described. However, these findings require a period of survival to develop—many cases, particularly if the decedent succumbs quickly, show no findings at all. The diagnosis of hypothermia therefore relies heavily on scene investigation. “Paradoxical undressing” (demonstrated in this case), refers to the phenomenon of a terminally hypothermic person taking off their clothes. This is caused by a feeling of warmth resulting from failure of vasoconstriction in the skin, and contributed by altered mentation.
Those at greatest risk are people spending extended time outdoors, including the homeless and outdoor recreationalists. The elderly and very young have a lower ability to centrally regulate body temperature. Children’s increased body surface area also leads to more rapid heat loss. People who are intoxicated with alcohol or drugs may not sense the cold or lack judgment to seek shelter. Alcohol also acts as a vasodilator, impairing vasoconstrictive adaptation to cold.
As the weather cools down, be mindful of how easily hypothermia can develop. Temperatures can be above freezing, yet those who are vulnerable are still at risk of hypothermia. Prepare yourself well for any snowy excursions, and keep an eye on those in your community who may not be able to seek shelter.

known as Wischnewsky spots. These are not specific to hypothermia and may just be an indicator of physiologic stress.


-Alison Krywanczyk, MD, FASCP, is currently a Deputy Medical Examiner at the Cuyahoga County Medical Examiner’s Office.
