Case History
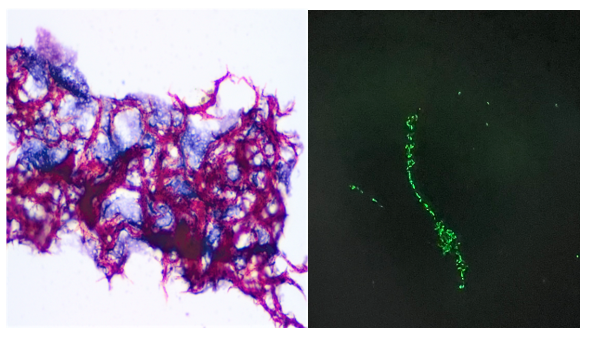
A 74-year-old female from El Salvador with a medical history of hypertension, diabetes, osteoarthritis presented with persistent productive cough. The patient states that the symptoms started on November 2022 which was believed to be associated with ongoing COVID-19 infection. Despite recovery from COVID-19 infection, significant productive cough still remained. A visit to her primary care doctor revealed streptococcal throat infection and despite completing a course of Zithromax antibiotics, a subsequent chest x-ray revealed potential right upper lobe pneumonia and she reported productive cough with occasional blood streaks. Blood work up in the Emergency Department revealed leukocytosis (20.22 x10e3/mcL) with neutrophilia (14.56 x10e3/mcL neutrophils) and monocytosis (3.03 x10e3/mcL monocytes). A chest x-ray showed bilateral reticular and airspace opacities with an air-fluid level containing opacity overlying the left mid lung, likely representing a cavitary lesion. A follow up with a computerized tomography of the chest identified innumerable randomly distributed pulmonary nodules or cavities with upper lobe predominance. The largest cavity measures approximately 6.6 cm with air-fluid levels and debris. Additionally, a small pericardial effusion with thickened pericardium was also noted. A sputum sample was submitted for Acid-fast bacilli (AFB) culture and molecular testing. AFB stain was positive for acid-fast bacilli (Figure 1). The GeneXpert MTB/RIF assay detected M. tuberculosis with no rifampin resistance marker. Growth on the Lowenstein-Jensen agar after two weeks showed buff colored rough and dry colonies and was confirmed as M. tuberculosis on the MALDI-TOF.
Discussion
Mycobacteria are aerobic, nonmotile, thin rod shape, non-spore forming bacilli that possess mycolic acid in its cell wall giving its acid-fast stain characteristics. Tuberculosis (TB) is an airborne disease caused by Mycobacterium tuberculosis (MTB). TB remains to be the leading cause of death from a single infectious agent worldwide. According to the CDC a total of 1.6 million people died from TB in 2021 (including 187, 000 people with HIV) 1,2. The M. tuberculosis complex (MTBC) includes M. tuberculosis, M. bovis, M. bovis, Bacille Calmette-Guérin strain (BCG), M. caprae, M. pinnipedii, M. mungi,M. africanum, M. microti, and M. canettii 3. M. tuberculosis produces cord factor, a glycolipid which is also known as trehalose dimycolate, that causes the bacteria to grow in parallel strands and that appeared like cord, or rope when cultured in liquid media (Figure 1A). The cord factor is present in the outer envelope and protects the bacteria from the host response 4.
The pathogenesis of human tuberculosis involves a complex interaction between host immune system and bacterial factors 4. M. tuberculosis is carried in airborne particles generated by infected individuals. The droplet nuclei traverse the mouth or nasal passages, upper respiratory tract, and bronchi to reach the alveoli of the lungs. The bacteria are then phagocytosed by alveolar macrophages and can inhibit maturation of phagosome and block formation of phagolysosome, allowing its unchecked replication in the macrophage which results in bacteria proliferation in the alveolar macrophage and air spaces. In immunocompetent hosts, the immune response (via TLR2, TLR9, Th-1 and IFN- ꝩ cascades) may contain the infection before significant tissue destruction or systemic illness 1-4. However, in the immunosuppressed hosts, the primary infection results in a broad clinical spectrum such as meningitis, miliary tuberculosis and extrapulmonary granulomas. Post-primary/secondary tuberculosis (reactivation TB) usually begins months to years after the establishment of systemic immunity in primary TB mostly in a period when the host immune response is weakened, following exogenous or a large inoculum of virulent bacilli overwhelming the host immunity system. Extrapulmonary manifestations will develop based on the organ system affected 5.HIV infection is the greatest risk factor for reactivation of TB as the virus causes functional abnormalities in CD4+ T cells and CD8+ T cells which confer protection against active TB. Other risk factors that promote the reactivation TB include aging, malnutrition, diabetes mellitus, renal failure, cancer and immunosuppressive therapy 5. The disease typically affects the lungs (pulmonary TB) but can affect other sites as regional lymph nodes, apex of the lung, larynx, kidneys, brain, bone, joints and pleura 1,2,5.
Diagnostic tests for TB detect either the bacteria or host immune response. Specimens recommended for diagnosis of mycobacterial infection are sputum, bronchial brushing/washings /biopsies, gastric aspirates (children) urine, blood, CSF, BM, body fluids, stool (only in HIV) 5,8. Specimens from sputum and other nonsterile sites should be liquefied with N-acetyl-L-cysteine and decontaminated with NaOH and for gastric aspirate neutralized with buffer 6-8. For diagnostic purposes, all persons suspected of having TB disease at any site should have at least three consecutive sputum specimens collected in 8 to 24 hours with at least one being an early morning one for AFB smear and culture 1,8.
The organisms can be visualized under a microscope using two principal methods: carbolfuchsin staining (e.g., Acid-fast stain), or using a fluorochrome (auramine-rhodamine and auramine-O stains) procedure (Figure 1B). Microscopy is the most rapid diagnostic method for the detection of tubercle bacilli but is less sensitive; it requires a minimum of 10,000 bacilli/mL of sputum to produce a positive result. Culture is the gold standard and more sensitive method for the detection of tubercle bacilli and is necessary for performing antimicrobial drug drug-susceptibility testing and genotyping. 6,9 However culture requires 3–6 weeks for growth which delays the initiation of anti-tuberculosis drug therapy. Two types of solid media are used for mycobacterial culture: egg based (Löwenstein-Jensen) and agar based (Middlebrook 7H10, 7H11, and selective 7H11). Colony morphology of Mycobacterium tuberculosis on solid media are dry, rough, raised, wrinkled, off white to buff colored. M. tuberculosis is commonly positive for niacin, nitrate reduction test, pyrazinamidase test, but negative for 68C catalase, tween 80 hydrolysis, and 5% NaCl tolerance. Molecular techniques such as nucleic acid amplification tests revolutionized tuberculosis diagnosis since M. tuberculosis nucleic acid material can be detected directly from specimen in less than 2 hours. Two commercial NAATs for the detection of M. tuberculosis complex are available in the United States: The Amplified MTD (Mycobacterium Tuberculosis Direct) test (Hologic, Marlborough, MA) and the Xpert MTB/RIF (Cepheid, Sunnyvale, CA).
Common serological approaches for detection of M. tuberculosis are the Tuberculin skin test (TST) or IFN- ꝩ release assays (IGRA’s) 1,9,10. The tuberculin skin test is performed by intracutaneous injection of purified protein derivative of M. tuberculosis, which induces a visible and palpable induration that peaks in 48 to 72 hours. A false-positive tuberculin skin test may result on individuals with prior vaccination with BCG (Bacillus Calmette-Guerin), an attenuated strain of M. bovis. BCG immunization does not affect the test result of IGRA assay. The IGRA are blood tests that measure a person’s immune reactivity to M. tuberculosis. Both T-Spot and QuantiFERON can aid in diagnosis M. tuberculosis but do not differentiate latent infection from tuberculosis disease. IGRAs are in vitro tests that measure the IFN- γ production by T cells responding to stimulation with specific TB antigens ESAT-6, TB7.7, and CFP-10, which are not present in the M. bovis strains. Results can be interpreted both qualitatively (positive, negative, or indeterminate) and quantitatively.
The regimen currently recommended for treatment of TB is isoniazid, rifampin, ethambutol, and pyrazinamide. The initial M. tuberculosis isolate should be tested for resistance to first-line medication. Second-line drug susceptibility testing should be limited to specimens from patients who have prior TB disease treatment, contact with a patient with known TB drug resistance or positive cultures after more than 3 months of treatment 10. Multidrug-resistant TB (MDR TB) disease is defined as resistance to isoniazid and rifampin, and Extensively drug-resistant TB (XDR TB) is characterized with resistance to isoniazid and rifampin, any fluoroquinolone, and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin). The duration of therapy depends on the drugs used, the drug susceptibility test results, and the patient’s response to therapy. Most patients are started with a 6-month regimen plan. A difficult challenge to M. tuberculosis treatment is patient compliance with lengthened therapy. Without treatment mortality rate for tuberculosis is more than 50% 11.
References
- World Health Organization, Global TB Programme. Global tuberculosis report 2022. 2022 November 19. https://www.who.int/publications/i/item/9789240061729
- Kamholz, S. L. 1996. Pleural tuberculosis, p. 483-491. In W. N. Rom and S. Garay (ed.), Tuberculosis. Little, Brown and Co., Boston, Mass.
- Yanti, B., et al. The role of Mycobacterium tuberculosis complex species on apoptosis and necroptosis state of macrophages derived from active pulmonary tuberculosis patients. BMC Res Notes. 2020; 13: 415. doi: 10.1186/s13104-020-05256-2
- Smith, Issar. Mycobacterium tuberculosis Pathogenesis and Molecular Determinants of Virulence Clin Microbiol Rev. 2003 Jul; 16(3): 463–496. doi: 10.1128/CMR.16.3.463-496.2003
- Wells, C.D, et al. HIV infection and multidrug-resistant tuberculosis: the perfect storm. J Infect Dis. 2007 Aug 15;196 Suppl 1:S86-107. doi: 10.1086/518665.
- Dunn, J.J., Starke, J.R., Revell, P.A. Laboratory Diagnosis of Mycobacterium tuberculosis Infection and Disease in Children. J Clin Microbiol 2016 Jun;54(6):1434-1441. doi: 10.1128/JCM.03043-15.
- Parashar D, Kabra S, Lodha R, Singh V, Mukherjee A, Arya T, Grewal H, Singh S. 2013. Does neutralization of gastric aspirates from children with suspected intrathoracic tuberculosis affect mycobacterial yields on MGIT culture? J Clin Microbiol 51:1753–1756.
- Clinical and Laboratory Standards Institute. 2008. Laboratory detection and identification of mycobacteria; approved guideline—1st edition. CLSI document M48-A. Clinical and Laboratory Standards Institute, Wayne, PA.
- Pai M, Nicol MP, Boehme CC. Tuberculosis Diagnostics: State of the Art and Future Directions. Microbiol Spectr 2016; 4.
- Dheda, K. et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. 2017 Mar 15;S2213-2600(17)30079-6.
- World Health Organization. Tuberculosis Fact Sheet. 21 April 2023. https://www.who.int/news-room/fact-sheets/detail/tuberculosis

-Dr. Carla Ayala-Soriano was born and raised in Bayamon, Puerto Rico. She attended Universidad Autonoma de Guadalajara School of Medicine where she received her doctorate degree. She completed a Bachelor of Science in Biology at the University of Puerto Rico. She spent an additional year completing a Post Bachelor Certificate in Cytotechnology. Her academic interests include Cytopathology and Gynecologic Pathology. In her spare time, Dr. Ayala-Soriano enjoys cooking, traveling, listen to music, and outdoor activities. She is pursuing AP/CP training.

-Rebecca Yee, PhD, D(ABMM), M(ASCP)CM is the Chief of Microbiology, Director of Clinical Microbiology and Molecular Microbiology Laboratory at the George Washington University Hospital. Her interests include bacteriology, antimicrobial resistance, and development of infectious disease diagnostics.
