An 81 year old female presented to the head and neck clinic after being diagnosed with cutaneous T cell lymphoma of the posterior mid-parietal scalp at an outside institution. She was initially treated with Brentuximab every three weeks but developed significant toxicities. The patient’s previous “T cell lymphoma” material was reviewed at our institution and the immunophenotypic report described the neoplastic cells as being positive for CD45, CD2, CD4, BCL6+, CD3 (subset), and CD123 (scattered), while negative for CD7, CD8, CD20, CD30, CD56, EBER ISH, PAX5, and lysozyme. Immunohistochemical slides were not provided for review. Flow cytometric analysis determined that there was no immunophenotypic evidence of a clonal T cell population in the patient’s peripheral blood.
A second scalp biopsy was performed at another outside institution, and the findings were similar to the parietal scalp; however, there were atypical pleomorphic cells which displayed irregular contours, hyperchromasia, and multiple nucleoli. The atypical cells were predominantly positive for CD4 and diffuse positivity for CD1a. These same pleomorphic cells were negative for CD3, CD8, CD20, CD30, ALK1, BCL6, CD56, EBER, AE1/AE3, SOX10, Desmin, PAX5, MUM1, CD5, and Cam 5.2.
The smears contained large, highly pleomorphic cells with irregular, elongated, and multilobated nuclei, frequent nuclear grooves and folds, fine chromatin, prominent nucleoli, and variable amounts of pale, eosinophilic cytoplasm, alt.
The outside tissue block on the original scalp biopsy was requested, and our pathology department performed additional immunostains. The neoplastic cells of interest were positive for CD1a, S100, CD68 (a small subset), and negative for lysozyme, CD21, CD30, and CD3. Ki67 proliferation index was interpreted at approximately 60%. An unstained FFPE tissue section was sent to a reference laboratory, and the neoplastic cells were strongly positive for Langerin.
While the Brentuximab treatment initially appeared to have a positive impact on the overall disease burden, the PET CT following 3 cycles showed a mixed response, including resolution of cervical lymphadenopathy and identification of multiple new lung nodules and bulky mediastinal lymphadenopathy. Between that and numerous reported toxicities, the treatment protocol was discontinued. The patient was then referred to radiology for a CT-scan guided right lower lobe lung biopsy measuring 2.2 x 1.3 centimeters with an SUV or 29.6.
In the CT Scan suite, we received multiple FNA passes from the interventional radiologist and made air-dried and alcohol-fixed smears, rinsing the residual needle material into a tube of balanced salt solution for a cell block preparation. We determined our specimen was adequate for scant tumor cells, as depicted on the Diff-Quik smears below.
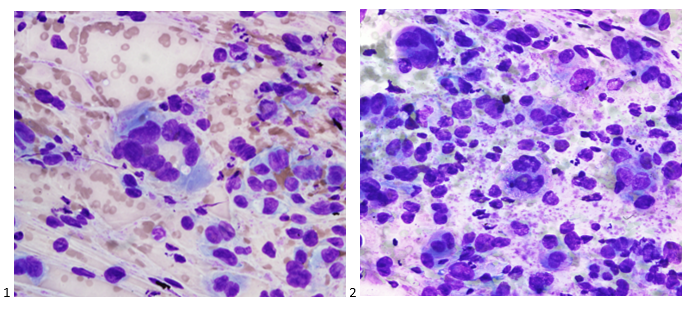
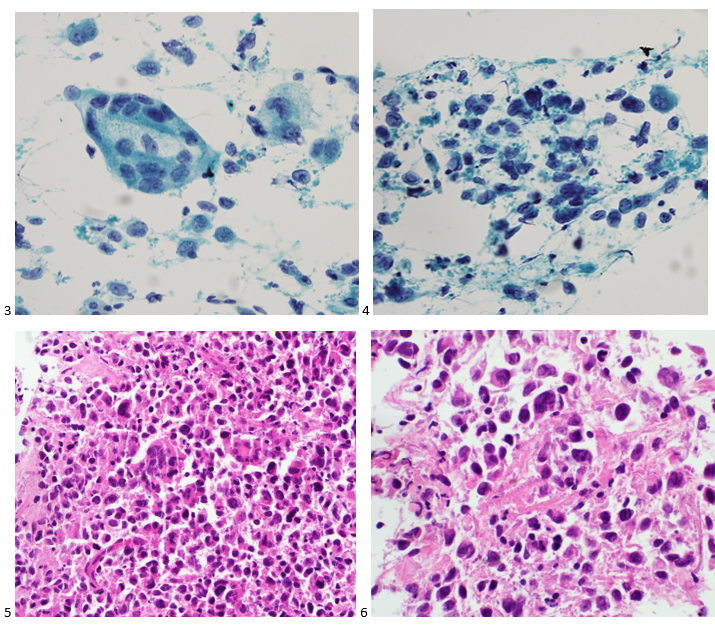
In comparison to the material from the second scalp biopsy, the cells from the lung biopsy appeared identical. Our Pap-stained smears and H&E cell block sections also demonstrated the highly pleomorphic cells described above.
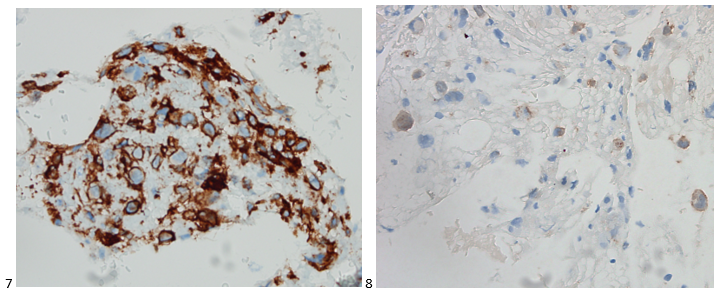
Immunostains performed on the cell block slides with adequate controls show that the tumor cells are positive for CD1a, CD4, partially positive for CD45 and S100, negative for AE1/3, TTF-1, and p40.
Our pathologists felt the cells from the second scalp biopsy and the lung biopsy were representative of a Langerhans cell sarcoma, a form of malignant histiocytosis, rather than a T-cell lymphoma. It is possible that the first scalp biopsy’s diagnosis of T-cell lymphoma was due to sampling error and the pleomorphic cells of interest were missed. The Ki-67 proliferative index of 60% helped to distinguish between Langerhans cell histiocytosis and Langerhans cell sarcoma.
Molecular testing performed on the core biopsy was negative for a BRAF mutation and positive for an NF1 inactivating mutation. The tumor may then be sensitive to mTOR inhibitors and MAPK pathway inhibitors, such as MEK inhibitors. Appeals for a MEK inhibitor were denied by insurance, but fortunately, the tumor also demonstrated high PD-L1 expression at 90%, making this specific patient a candidate for pembrolizumab, which was fully covered by insurance.
____________________________________________________________________________________________
I can’t help but think about the disparities associated with cancer and the inaccessibility of potentially lifesaving or life-prolonging treatments. Sure, there may be viable alternatives, such as this case, but what if we had equal access to cutting edge, personalized therapies? What if the only therapy available was too costly to bear? Just because a cancer might be rare, such as Langerhans cell sarcoma, it doesn’t mean access to a proven effective therapy should also be rare. Even with drug assistance programs, so many patients face the harsh reality of tapping into their life savings to just to save their own life. When we became medical laboratory professionals, we promised to provide timely and accurate for all of our patients. Now, it’s time that pharmaceutical companies and our healthcare system as a whole work together to provide high quality, low-cost, readily accessible and personalized treatment options to every patient. They deserve that chance to overcome or at least manage their cancer.

-Taryn Waraksa-Deutsch, MS, SCT(ASCP)CM, CT(IAC), has worked as a cytotechnologist at Fox Chase Cancer Center, in Philadelphia, Pennsylvania, since earning her master’s degree from Thomas Jefferson University in 2014. She is an ASCP board-certified Specialist in Cytotechnology with an additional certification by the International Academy of Cytology (IAC). She is also a 2020 ASCP 40 Under Forty Honoree.
